Гипералгезия
| Гипералгезия | |
|---|---|
 | |
| Специальность | Неврология |
Hyperalgesia ( / ˌ H aɪ p ər æ l ˈ dʒ iː z i ə / или / - s i ə / ; гипер от греческого ὑπέρ ( huper ) 'over' + -лгезия от греческой ἄλγος (алго Ненормально повышенная чувствительность к боли , которая может быть вызвана повреждением ноцицепторов или периферических нервов и может вызвать гиперчувствительность к стимулу. Простагландины E и F несут в основном ответственность за сенсибилизацию ноцицепторов. [ 1 ] Временная повышенная чувствительность к боли также возникает в рамках поведения болезни , развитый ответ на инфекцию. [ 2 ]
Типы
[ редактировать ]Гипералгезия может возникнуть в фокусах, дискретных областях или в виде более диффузной формы всего тела. Исследования кондиционирования установили, что можно испытать научную гипералгезию последней диффузной формы.
Форма фокус обычно связана с травмой и делится на два подтипа:
- Первичная гипералгезия описывает чувствительность к боли, которая возникает непосредственно в поврежденных тканях.
- Secondary hyperalgesia describes pain sensitivity that occurs in surrounding undamaged tissues.
Opioid-induced hyperalgesia may develop as a result of long-term opioid use in the treatment of chronic pain.[3] Various studies of humans and animals have demonstrated that primary or secondary hyperalgesia can develop in response to both chronic and acute exposure to opioids. This side effect can be severe enough to warrant discontinuation of opioid treatment.
Causes
[edit]Hyperalgesia is induced by platelet-activating factor (PAF) which comes about in an inflammatory or an allergic response. This seems to occur via immune cells interacting with the peripheral nervous system and releasing pain-producing chemicals (cytokines and chemokines).[4]
One unusual cause of focal hyperalgesia is platypus venom.[5]
Long-term opioid (e.g. heroin, morphine) users and those on high-dose opioid medications for the treatment of chronic pain, may experience hyperalgesia and experience pain out of proportion to physical findings, which is a common cause for loss of efficacy of these medications over time.[3][6][7] As it can be difficult to distinguish from tolerance, opioid-induced hyperalgesia is often compensated for by escalating the dose of opioid, potentially worsening the problem by further increasing sensitivity to pain. Chronic hyperstimulation of opioid receptors results in altered homeostasis of pain signalling pathways in the body with several mechanisms of action involved. One major pathway being through stimulation of the nociceptin receptor,[8][9][10] and blocking this receptor may therefore be a means of preventing the development of hyperalgesia.[11]
Stimulation of nociceptive fibers in a pattern consistent with that from inflammation switches on a form of amplification in the spinal cord, long term potentiation.[12] This occurs where the pain fibres synapse to pain pathway, the periaqueductal grey. Amplification in the spinal cord may be another way of producing hyperalgesia.
The release of proinflammatory cytokines such as interleukin-1 by activated leukocytes triggered by lipopolysaccharides, endotoxins and other signals of infection also increases pain sensitivity as part of sickness behavior, the evolved response to illness.[2][13][14]
Diagnosis
[edit]Simple bedside tests include response (pain intensity and character) to cotton swab, finger pressure, pinprick, cold and warm stimuli, e.g., metal thermo rollers at 20°C and 40°C, as well as mapping of the area of abnormality.[citation needed]
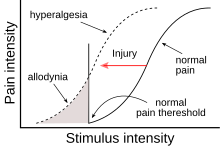
Quantitative sensory testing can be used to determine pain thresholds (decreased pain threshold indicates allodynia) and stimulus/response functions (increased pain response indicate hyperalgesia). Dynamic mechanical allodynia can be assessed using a cotton swab or a brush. A pressure algometer and standardized monofilaments or weighted pinprick stimuli are used for assessing pressure and punctate allodynia and hyperalgesia and a thermal tester is used for thermal testing.[15][16]
Treatment
[edit]Hyperalgesia is similar to other sorts of pain associated with nerve irritation or damage such as allodynia and neuropathic pain, and consequently may respond to standard treatment for these conditions, using various drugs such as SSRI or tricyclic antidepressants,[17][18] Nonsteroidal anti-inflammatory drugs (NSAIDs),[19] glucocorticoids,[20] gabapentin[21] or pregabalin,[22] NMDA antagonists,[23][24][25] or atypical opioids such as tramadol.[26] Where hyperalgesia has been produced by chronic high doses of opioids, reducing the dose may result in improved pain management.[27] However, as with other forms of nerve dysfunction associated pain, treatment of hyperalgesia can be clinically challenging, and finding a suitable drug or drug combination that is effective for a particular patient may require trial and error. The use of a transcutaneous electrical nerve stimulation device has been shown to alleviate hyperalgesia.[28][29]
See also
[edit]References
[edit]- ^ "Clinical Pharmacology". www.clinicalpharmacology-ip.com. Archived from the original on 2019-12-10. Retrieved 2017-06-25.
- ^ Jump up to: a b Hart BL (1988). "Biological basis of the behavior of sick animals". Neurosci Biobehav Rev. 12 (2): 123–37. doi:10.1016/S0149-7634(88)80004-6. PMID 3050629. S2CID 17797005.
- ^ Jump up to: a b Chu LF, Angst MS, Clark D (2008). "Opioid-induced hyperalgesia in humans: molecular mechanisms and clinical considerations". Clin J Pain. 24 (6): 479–96. doi:10.1097/AJP.0b013e31816b2f43. PMID 18574358. S2CID 8489213.
- ^ Marchand F, Perretti M, McMahon SB (July 2005). "Role of the immune system in chronic pain". Nat. Rev. Neurosci. 6 (7): 521–32. doi:10.1038/nrn1700. PMID 15995723. S2CID 9660194.
- ^ de Plater GM, Milburn PJ, Martin RL (March 2001). "Venom from the platypus, Ornithorhynchus anatinus, induces a calcium-dependent current in cultured dorsal root ganglion cells". J. Neurophysiol. 85 (3): 1340–45. doi:10.1152/jn.2001.85.3.1340. PMID 11248005. S2CID 2452708.
- ^ DuPen A, Shen D, Ersek M (September 2007). "Mechanisms of opioid-induced tolerance and hyperalgesia". Pain Manag Nurs. 8 (3): 113–21. doi:10.1016/j.pmn.2007.02.004. PMID 17723928.
- ^ Mitra S (2018). "Opioid-induced hyperalgesia: pathophysiology and clinical implications". J Opioid Manag. 4 (3): 123–30. doi:10.5055/jom.2008.0017. PMID 18717507.
- ^ Okuda-Ashitaka E, Minami T, Matsumura S, et al. (February 2006). "The opioid peptide nociceptin/orphanin FQ mediates prostaglandin E2-induced allodynia, tactile pain associated with nerve injury". Eur. J. Neurosci. 23 (4): 995–1004. doi:10.1111/j.1460-9568.2006.04623.x. PMID 16519664. S2CID 39006891.
- ^ Fu X, Zhu ZH, Wang YQ, Wu GC (January 2007). "Regulation of proinflammatory cytokines gene expression by nociceptin/orphanin FQ in the spinal cord and the cultured astrocytes". Neuroscience. 144 (1): 275–85. doi:10.1016/j.neuroscience.2006.09.016. PMID 17069983. S2CID 40500310.
- ^ Chen Y, Sommer C (May 2007). "Activation of the nociceptin opioid system in rats. Sensory neurons produce antinociceptive effects in inflammatory pain: involvement of inflammatory mediators" (PDF). J. Neurosci. Res. 85 (7): 1478–88. doi:10.1002/jnr.21272. hdl:10161/13662. PMID 17387690. S2CID 41843938.[permanent dead link]
- ^ Tamai H, Sawamura S, Takeda K, Orii R, Hanaoka K (March 2005). "Anti-allodynic and anti-hyperalgesic effects of nociceptin receptor antagonist, JTC-801, in rats after spinal nerve injury and inflammation". Eur. J. Pharmacol. 510 (3): 223–28. doi:10.1016/j.ejphar.2005.01.033. PMID 15763246.
- ^ Ikeda H, Stark J, Fischer H, et al. (June 2006). "Synaptic amplifier of inflammatory pain in the spinal dorsal horn". Science. 312 (5780): 1659–62. Bibcode:2006Sci...312.1659I. doi:10.1126/science.1127233. PMID 16778058. S2CID 20540556.
- ^ Kelley KW, Bluthé RM, Dantzer R, et al. (February 2003). "Cytokine-induced sickness behavior". Brain Behav. 17 (Suppl 1): S112–18. doi:10.1016/S0889-1591(02)00077-6. PMID 12615196. S2CID 25400611.
- ^ Maier SF, Wiertelak EP, Martin D, Watkins LR (October 1993). "Interleukin-1 mediates the behavioral hyperalgesia produced by lithium chloride and endotoxin". Brain Res. 623 (2): 321–24. doi:10.1016/0006-8993(93)91446-Y. PMID 8221116. S2CID 40529634.
- ^ Haanpää M, Attal N, Backonja M, Baron R, Bennett M, Bouhassira D, Cruccu G, Hansson P, Haythornthwaite JA, Iannetti GD, Jensen TS, Kauppila T, Nurmikko TJ, Rice AS, Rowbotham M, Serra J, Sommer C, Smith BH, Treede RD (Jan 2001). "NeuPSIG guidelines on neuropathic pain assessment". Pain. 152 (1): 14–27. doi:10.1016/j.pain.2010.07.031. PMID 20851519. S2CID 2032474.
- ^ Jensen TS, Finnerup NB (Sep 2014). "Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms". Lancet Neurol. 13 (9): 924–35. doi:10.1016/S1474-4422(14)70102-4. PMID 25142459. S2CID 25011309.
- ^ Sindrup SH, Otto M, Finnerup NB, Jensen TS (June 2005). "Antidepressants in the treatment of neuropathic pain". Basic & Clinical Pharmacology & Toxicology. 96 (6): 399–409. doi:10.1111/j.1742-7843.2005.pto_96696601.x. PMID 15910402.
- ^ Matsuzawa-Yanagida K, Narita M, Nakajima M, et al. (July 2008). "Usefulness of antidepressants for improving the neuropathic pain-like state and pain-induced anxiety through actions at different brain sites". Neuropsychopharmacology. 33 (8): 1952–65. doi:10.1038/sj.npp.1301590. PMID 17957217.
- ^ Koppert W, Wehrfritz A, Körber N, et al. (March 2004). "The cyclooxygenase isozyme inhibitors parecoxib and paracetamol reduce central hyperalgesia in humans". Pain. 108 (1–2): 148–53. doi:10.1016/j.pain.2003.12.017. PMID 15109518. S2CID 33124447.
- ^ Stubhaug A, Romundstad L, Kaasa T, Breivik H (October 2007). "Methylprednisolone and Ketorolac rapidly reduce hyperalgesia around a skin burn injury and increase pressure pain thresholds". Acta Anaesthesiol Scand. 51 (9): 1138–46. doi:10.1111/j.1399-6576.2007.01415.x. PMID 17714578. S2CID 20639496.
- ^ Gottrup H, Juhl G, Kristensen AD, et al. (December 2004). "Chronic oral Gabapentin reduces elements of central sensitization in human experimental Hyperalgesia". Anesthesiology. 101 (6): 1400–08. doi:10.1097/00000542-200412000-00021. PMID 15564948. S2CID 15060257.
- ^ Chizh BA, Göhring M, Tröster A, Quartey GK, Schmelz M, Koppert W (February 2007). "Effects of oral pregabalin and aprepitant on pain and central sensitization in the electrical hyperalgesia model in human volunteers". Br J Anaesth. 98 (2): 246–54. doi:10.1093/bja/ael344. PMID 17251214.
- ^ Warncke T, Stubhaug A, Jørum E (August 1997). "Ketamine, an NMDA receptor antagonist, suppresses spatial and temporal properties of burn-induced secondary Hyperalgesia in man: a double-blind, cross-over comparison with morphine and placebo". Pain. 72 (1–2): 99–106. doi:10.1016/S0304-3959(97)00006-7. PMID 9272793. S2CID 1343794.
- ^ De Kock MF, Lavand'homme PM (March 2007). "The clinical role of NMDA receptor antagonists for the treatment of postoperative pain". Best Pract Res Clin Anaesthesiol. 21 (1): 85–98. doi:10.1016/j.bpa.2006.12.006. PMID 17489221.
- ^ Klein T, Magerl W, Hanschmann A, Althaus M, Treede RD (January 2008). "Antihyperalgesic and analgesic properties of the N-methyl-D-aspartate (NMDA) receptor antagonist neramexane in a human surrogate model of neurogenic Hyperalgesia". Eur J Pain. 12 (1): 17–29. doi:10.1016/j.ejpain.2007.02.002. PMID 17449306. S2CID 2875679.
- ^ Кристоф Т., Кёгель Б., Страссбургер В., Шуг С.А. (2007). «Трамадол имеет лучшее соотношение потенции по сравнению с морфином в невропатических моделях, чем в моделях ноцицептивной боли». Наркотики в НИОКР . 8 (1): 51–57. doi : 10.2165/00126839-200708010-00005 . PMID 17249849 . S2CID 10268544 .
- ^ Vorobeychik Y, Chen L, Bush MC, Mao J (сентябрь 2008 г.). «Улучшенный опиоидный анальгетический эффект после снижения опиоидной дозы» . Обезболивающая медицина . 9 (6): 724–27. doi : 10.1111/j.1526-4637.2008.00501.x . PMID 18816332 .
- ^ Десантана, JM; Уолш, DM; Вэнс, c; Ракель, Б.А.; Слука, Ка (декабрь 2008 г.). «Эффективность чрескожной электрической нервной стимуляции для лечения гипералгезии и боли» . Текущие ревматологические отчеты . 10 (6): 492–99. doi : 10.1007/s11926-008-0080-z . PMC 2746624 . PMID 19007541 .
- ^ Слука, Ка; Чандран, P (ноябрь 2002 г.). «Усиленное снижение гипералгезии путем комбинированного введения клонидина и десятков». Боль . 100 (1–2): 183–90. doi : 10.1016/s0304-3959 (02) 00294-4 . PMID 12435471 . S2CID 12117342 .