Фибромиалгия
| Фибромиалгия | |
|---|---|
| Другие имена | Синдром фибромиалгии |
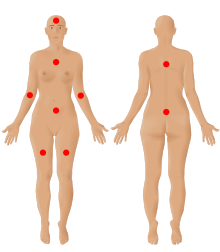 | |
| Девять возможных боли в фибромиалгии в соответствии с Американским обществом боли . | |
| Произношение | |
| Специальность | Ревматология , неврология [ 2 ] |
| Symptoms | Widespread pain, feeling tired, sleep problems[3][4] |
| Usual onset | Early-Middle age[5] |
| Duration | Long term[3] |
| Causes | Unknown[4][5] |
| Diagnostic method | Based on symptoms after ruling out other potential causes[4][5] |
| Differential diagnosis | Anemia, autoimmune disorders (such as ankylosing spondylitis, polymyalgia rheumatica, rheumatoid arthritis, scleroderma, or multiple sclerosis), Lyme disease, osteoarthritis, thyroid disease[6][7] |
| Treatment | Sufficient sleep and exercise[5] |
| Medication | Duloxetine, milnacipran, pregabalin, gabapentin[5][8] |
| Prognosis | Normal life expectancy[5] |
| Frequency | 2%[4] |
Фибромиалгия - это медицинский синдром , который вызывает хроническую широко распространенную боль , сопровождаемая усталостью , пробуждением без каких -либо оттенков и когнитивными симптомами . Другие симптомы могут включать головные боли , боль в нижней части живота или судороги , а также депрессию . [ 9 ] Люди с фибромиалгией также могут испытать бессонницу [ 10 ] и общая гиперчувствительность . [ 11 ] [ 12 ] Причина фибромиалгии неизвестна, но, как полагают, включает в себя комбинацию генетических факторов и факторов окружающей среды. [ 4 ] Факторы окружающей среды могут включать психологический стресс , травму и определенные инфекции . [ 4 ] Поскольку боль, по -видимому, является результатом процессов в центральной нервной системе , это состояние называется «синдромом центральной сенсибилизации». [ 4 ] [ 13 ]
Фибромиалгия была впервые определена в 1990 году с обновленными критериями в 2011 году, [ 4 ] 2016, [ 9 ] 2019. [ 12 ] Термин «фибромиалгия» взят из нео-латиновой фибро- , что означает «волокнистые ткани», греческие μυο- мио- , «мышцы» и греческие алгоироды άλγος , «боль»; Таким образом, термин буквально означает « мышечную и волокнистую боль в соединении ». [ 14 ] Fibromyalgia is estimated to affect 2–4% of the population.[15] Women are affected about twice as often as men.[4][15] Rates appear similar in different areas of the world and among different cultures.[4]
The treatment of fibromyalgia is symptomatic[16] and multidisciplinary.[17] The European Alliance of Associations for Rheumatology strongly recommends aerobic and strengthening exercise.[17] Weak recommendations are given to mindfulness, psychotherapy, acupuncture, hydrotherapy, and meditative exercise such as qigong, yoga, and tai chi.[17] The use of medication in the treatment of fibromyalgia is debated[17][18] although antidepressants can improve quality of life.[19] Common helpful medications include other serotonin–norepinephrine reuptake inhibitors, nonsteroidal anti-inflammatory drugs, and muscle relaxants.[20] Q10 coenzyme and vitamin D supplements may reduce pain and improve quality of life.[21] While fibromyalgia is persistent in nearly all patients, it does not result in death or tissue damage.[18]
History
[edit]Chronic widespread pain had already been described in the literature in the 19th century but the term fibromyalgia was not used until 1976 when Dr P.K. Hench used it to describe these symptoms.[22] Many names, including muscular rheumatism, "fibrositis", "psychogenic rheumatism", and "neurasthenia" were applied historically to symptoms resembling those of fibromyalgia.[23] The term fibromyalgia was coined by researcher Mohammed Yunus as a synonym for fibrositis and was first used in a scientific publication in 1981.[24] Fibromyalgia is from the Latin fibra (fiber)[25] and the Greek words myo (muscle)[26] and algos (pain).[27]
Historical perspectives on the development of the fibromyalgia concept note the "central importance" of a 1977 paper by Smythe and Moldofsky on fibrositis.[28][29] The first clinical, controlled study of the characteristics of fibromyalgia syndrome was published in 1981,[30] providing support for symptom associations. In 1984, an interconnection between fibromyalgia syndrome and other similar conditions was proposed,[31] and in 1986, trials of the first proposed medications for fibromyalgia were published.[31]
A 1987 article in the Journal of the American Medical Association used the term "fibromyalgia syndrome" while saying it was a "controversial condition".[32] The American College of Rheumatology (ACR) published its first classification criteria for fibromyalgia in 1990.[33] Later revisions were made in 2010,[34] 2016,[9] and 2019.[12]
Classification
[edit]Fibromyalgia is classed as a disorder of pain processing due to abnormalities in how pain signals are processed in the central nervous system.[35] The International Classification of Diseases (ICD-11) includes fibromyalgia in the category of "Chronic widespread pain," code MG30.01.[36] People with fibromyalgia differ in several dimensions: severity, adjustment, symptom profile, psychological profile and response to treatment.[37]
Signs and symptoms
[edit]The defining symptoms of fibromyalgia are chronic widespread pain, fatigue, and sleep disturbance.[12] Other symptoms may include heightened pain in response to tactile pressure (allodynia),[12] cognitive problems,[12] musculoskeletal stiffness,[12] environmental sensitivity,[12] hypervigilance,[12] sexual dysfunction,[38] and visual symptoms.[39] Some people with fibromyalgia experience post-exertional malaise, in which symptoms flare up a day or longer after physical exercise.[40]
Pain
[edit]Fibromyalgia is predominantly a chronic pain disorder.[12] According to the NHS, widespread pain is one major symptom, which could feel like an ache, a burning sensation, or a sharp, stabbing pain.[41] Patients are also highly sensitive to pain, and the slightest touch can cause pain. Pain also tends to linger for longer when a patient experiences pain.[42]
Fatigue
[edit]Fatigue is one of the defining symptoms of fibromyalgia.[12] Patients may experience physical or mental fatigue. Physical fatigue can be demonstrated by a feeling of exhaustion after exercise or by a limitation in daily activities.[12]
Sleep problems
[edit]Sleep problems are a core symptom in fibromyalgia.[12] These include difficulty falling asleep or staying asleep, awakening while sleeping and waking up feeling unrefreshed.[12] A meta-analysis compared objective and subjective sleep metrics in people with fibromyalgia and healthy people. Individuals with fibromyalgia had lower sleep quality and efficiency, as well as longer wake time after sleep start, shorter sleep duration, lighter sleep, and greater trouble initiating sleep when objectively assessed, and more difficulty initiating sleep when subjectively assessed.[10] Sleep problems may contribute to pain by decreased release of IGF-1 and human growth hormone, leading to decreased tissue repair.[43] Improving sleep quality can help people with fibromyalgia minimize pain.[44][45]
Cognitive problems
[edit]Many people with fibromyalgia experience cognitive problems (known as fibrofog or brainfog). One study found that approximately 50% of fibromyalgia patients had subjective cognitive dysfunction and that it was associated with higher levels of pain and other fibromyalgia symptoms.[46] The American Pain Society recognizes these problems as a major feature of fibromyalgia, characterized by trouble concentrating, forgetfulness and disorganized or slow thinking.[12] About 75% of fibromyalgia patients report significant problems with concentration, memory, and multitasking.[47] A 2018 meta-analysis found that the largest differences between fibromyalgia patients and healthy subjects were for inhibitory control, memory, and processing speed.[47] It is hypothesized that the increased pain compromises attention systems, resulting in cognitive problems.[47]
Hypersensitivity
[edit]In addition to a hypersensitivity to pain, patients with fibromyalgia show hypersensitivity to other stimuli,[11] such as bright lights, loud noises, perfumes, and cold.[12] A review article found that they have a lower cold pain threshold.[48] Other studies documented an acoustic hypersensitivity.[49]
Comorbidity
[edit]Fibromyalgia as a stand-alone diagnosis is uncommon, as most fibromyalgia patients often have other chronic overlapping pain problems or mental disorders.[11] Fibromyalgia is associated with mental health issues like anxiety,[50] posttraumatic stress disorder,[4][50] bipolar disorder,[50] alexithymia,[51] and depression.[50][52][53] Patients with fibromyalgia are five times more likely to have major depression than the general population.[54] Experiencing pain and limited activity from having fibromyalgia leads to less activity, leading to social isolation and increased stress levels, which tends to cause anxiety and depression.[55]
Fibromyalgia and numerous chronic pain conditions frequently coexist.[52] These include chronic tension headaches,[50] myofascial pain syndrome,[50] and temporomandibular disorders.[50] Multiple sclerosis, post-polio syndrome, neuropathic pain, and Parkinson's disease are four neurological disorders that have been linked to pain or fibromyalgia.[52]
Fibromyalgia largely overlaps with several syndromes that may share the same pathogenetic mechanisms.[56][57] These include myalgic encephalomyelitis/chronic fatigue syndrome[58][56] and irritable bowel syndrome.[57]
Comorbid fibromyalgia has been reported to occur in 20–30% of individuals with rheumatic diseases.[52] It has been reported in people with noninflammatory musculoskeletal diseases.[52]
The prevalence of fibromyalgia in gastrointestinal disease has been described mostly for celiac disease[52] and irritable bowel syndrome (IBS).[52][50] IBS and fibromyalgia share similar pathogenic mechanisms, involving immune system mast cells, inflammatory biomarkers, hormones, and neurotransmitters such as serotonin. Changes in the gut biome alter serotonin levels, leading to autonomic nervous system hyperstimulation.[59]
Fibromyalgia has also been linked with obesity.[60] Other conditions that are associated with fibromyalgia include connective tissue disorders,[61] cardiovascular autonomic abnormalities,[62] obstructive sleep apnea-hypopnea syndrome,[63] restless leg syndrome[64] and an overactive bladder.[65]
Risk factors
[edit]The cause of fibromyalgia is unknown.[66][67] However, several risk factors, genetic and environmental, have been identified.
Genetics
[edit]Genetics play a major role in fibromyalgia, and may explain up to 50% of the disease susceptibility.[68] Fibromyalgia is potentially associated with polymorphisms of genes in the serotoninergic,[69] dopaminergic[69] and catecholaminergic systems.[69] Several genes have been suggested as candidates for susceptibility to fibromyalgia. These include SLC6A4,[68] TRPV2,[68] MYT1L,[68] NRXN3,[68] and the 5-HT2A receptor 102T/C polymorphism.[70] The heritability of fibromyalgia is estimated to be higher in patients younger than 50.[71]
Nearly all the genes suggested as potential risk factors for fibromyalgia are associated with neurotransmitters and their receptors.[72] Neuropathic pain and major depressive disorder often co-occur with fibromyalgia — the reason for this comorbidity appears to be due to shared genetic abnormalities, which leads to impairments in monoaminergic, glutamatergic, neurotrophic, opioid and proinflammatory cytokine signaling. In these vulnerable individuals, psychological stress or illness can cause abnormalities in inflammatory and stress pathways that regulate mood and pain. Eventually, a sensitization and kindling effect occurs in certain neurons leading to the establishment of fibromyalgia and sometimes a mood disorder.[73]
Stress
[edit]Stress may be an important precipitating factor in the development of fibromyalgia.[74] A 2021 meta-analysis found psychological trauma to be strongly associated with fibromyalgia.[75][76] People who suffered abuse in their lifetime were three times more likely to have fibromyalgia, people who suffered medical trauma or other stressors in their lifetime were about twice as likely.[75]
Some authors have proposed that, because exposure to stressful conditions can alter the function of the hypothalamic-pituitary-adrenal (HPA) axis, the development of fibromyalgia may stem from stress-induced disruption of the HPA axis.[77][78]
Personality
[edit]Although some have suggested that fibromyalgia patients are more likely to have specific personality traits, when depression is statistically controlled for, it appears that their personality is no different from that of people in the general population.[79]
Other risk markers
[edit]Other risk markers for fibromyalgia include premature birth, female sex, cognitive influences, primary pain disorders, multiregional pain, infectious illness, hypermobility of joints, iron deficiency and small-fiber polyneuropathy.[80] Metal-induced allergic inflammation has also been linked with fibromyalgia, especially in response to nickel but also inorganic mercury, cadmium, and lead.[81] Following the COVID-19 pandemic, some have suggested that the SARS-CoV-2 virus may trigger fibromyalgia.[82]
Pathophysiology
[edit]As of 2022, the pathophysiology of fibromyalgia has not yet been elucidated[83] and several theories have been suggested. The prevailing perspective considers fibromyalgia as a condition resulting from an amplification of pain by the central nervous system.[72] Substantial biological evidence backs up this notion, leading to the term of nociplastic pain.[72]
Fibromyalgia is associated with the deregulation of proteins in the complement and coagulation cascades as well as iron metabolism.[84] An excessive oxidative stress response may cause dysregulation of many proteins.[84]
Nervous system
[edit]Pain processing abnormalities
[edit]Chronic pain can be divided into three categories. Nociceptive pain is pain caused by inflammation or damage to tissues. Neuropathic pain is pain caused by nerve damage. Nociplastic pain (or central sensitization) is less understood and is the common explanation of the pain experienced in fibromyalgia.[13][15][85] Because the three forms of pain can overlap, fibromyalgia patients may experience nociceptive (e.g., rheumatic illnesses) and neuropathic (e.g., small fiber neuropathy) pain, in addition to nociplastic pain.[15]
Nociplastic pain (central sensitization)
[edit]Fibromyalgia can be viewed as a condition of nociplastic pain.[86] Nociplastic pain is caused by an altered function of pain-related sensory pathways in the periphery and the central nervous system, resulting in hypersensitivity.[87]
Nociplastic pain is commonly referred to as "Nociplastic pain syndrome" because it is coupled with other symptoms.[15] These include fatigue, sleep disturbance, cognitive disturbance, hypersensitivity to environmental stimuli, anxiety, and depression.[15] Nociplastic pain is caused by either (1) increased processing of pain stimuli or (2) decreased suppression of pain stimuli at several levels in the nervous system, or both.[15]
Neuropathic pain
[edit]An alternative hypothesis to nociplastic pain views fibromyalgia as a stress-related dysautonomia with neuropathic pain features.[88] This view highlights the role of autonomic and peripheral nociceptive nervous systems in the generation of widespread pain, fatigue, and insomnia.[89] The description of small fiber neuropathy in a subgroup of fibromyalgia patients supports the disease neuropathic-autonomic underpinning.[88] However, others claim that small fiber neuropathy occurs only in small groups of those with fibromyalgia.[18]
Autonomic nervous system
[edit]Some suggest that fibromyalgia is caused or maintained by a decreased vagal tone, which is indicated by low levels of heart rate variability,[74] signaling a heightened sympathetic response.[90] Accordingly, several studies show that clinical improvement is associated with an increase in heart rate variability.[91][90][92] Some examples of interventions that increase the heart rate variability and vagal tone are meditation, yoga, mindfulness and exercise.[74] In 2023 the Fibromyalgia: Imbalance of Threat and Soothing Systems (FITSS) model was suggested as a working hypothesis.[93] According to the FITSS model, the salience network (also known as the midcingulo-insular network) may remain continuously hyperactive due to an imbalance in emotion regulation, which is reflected by an overactive "threat" system and an underactive "soothing" system. This hyperactivation, along with other mechanisms, may contribute to fibromyalgia.[93]
Neurotransmitters
[edit]Some neurochemical abnormalities that occur in fibromyalgia also regulate mood, sleep, and energy, thus explaining why mood, sleep, and fatigue problems are commonly co-morbid with fibromyalgia.[35] Serotonin is the most widely studied neurotransmitter in fibromyalgia. It is hypothesized that an imbalance in the serotoninergic system may lead to the development of fibromyalgia.[94] There is also some data that suggests altered dopaminergic and noradrenergic signaling in fibromyalgia.[95] Supporting the monoamine related theories is the efficacy of monoaminergic antidepressants in fibromyalgia.[19] Glutamate/creatine ratios within the bilateral ventrolateral prefrontal cortex were found to be significantly higher in fibromyalgia patients than in controls, and may disrupt glutamate neurotransmission.[76][96]
Neurophysiology
[edit]Neuroimaging studies have observed that fibromyalgia patients have increased grey matter in the right postcentral gyrus and left angular gyrus, and decreased grey matter in the right cingulate gyrus, right paracingulate gyrus, left cerebellum, and left gyrus rectus.[97] These regions are associated with affective and cognitive functions and with motor adaptations to pain processing.[97] Other studies have documented decreased grey matter of the default mode network in people with fibromyalgia.[98] These deficits are associated with pain processing.[98]
Neuroendocrine system
[edit]Studies on the neuroendocrine system and HPA axis in fibromyalgia have been inconsistent. Depressed function of the HPA axis results in adrenal insufficiency and potentially chronic fatigue.[99]
One study found fibromyalgia patients exhibited higher plasma cortisol, more extreme peaks and troughs, and higher rates of dexamethasone non-suppression. However, other studies have only found correlations between a higher cortisol awakening response and pain, and not any other abnormalities in cortisol.[45] Increased baseline ACTH and increase in response to stress have been observed, hypothesized to be a result of decreased negative feedback.[95]
Oxidative stress
[edit]Pro-oxidative processes correlate with pain in fibromyalgia patients.[99] Decreased mitochondrial membrane potential, increased superoxide activity, and increased lipid peroxidation production are observed.[99] The high proportion of lipids in the central nervous system (CNS) makes the CNS especially vulnerable to free radical damage. Levels of lipid peroxidation products correlate with fibromyalgia symptoms.[99]
Immune system
[edit]Inflammation has been suggested to have a role in the pathogenesis of fibromyalgia.[100] People with fibromyalgia tend to have higher levels of inflammatory cytokines IL-6,[94][101][102] and IL-8.[94][101][102] There are also increased levels of the pro-inflammatory cytokines IL-1 receptor antagonist.[101][102] Increased levels of pro-inflammatory cytokines may increase sensitivity to pain, and contribute to mood problems.[103] Anti-inflammatory interleukins such as IL-10 have also been associated with fibromyalgia.[94]
A repeated observation shows that autoimmunity triggers such as traumas and infections are among the most frequent events preceding the onset of fibromyalgia.[104] Neurogenic inflammation has been proposed as a contributing factor to fibromyalgia.[105]
Digestive system
[edit]Gut microbiome
[edit]Though there is a lack of evidence in this area, it is hypothesized that gut bacteria may play a role in fibromyalgia.[106] People with fibromyalgia are more likely to show dysbiosis, a decrease in microbiota diversity.[107] There is a bidirectional interplay between the gut and the nervous system. Therefore, the gut can affect the nervous system, but the nervous system can also affect the gut. Neurological effects mediated via the autonomic nervous system as well as the hypothalamic pituitary adrenal axis are directed to intestinal functional effector cells, which in turn are under the influence of the gut microbiota.[108]
Gut-brain axis
[edit]The gut-brain axis, which connects the gut microbiome to the brain via the enteric nervous system, is another area of research. Fibromyalgia patients have less varied gut flora and altered serum metabolome levels of glutamate and serine,[109] implying abnormalities in neurotransmitter metabolism.[104]
Energy metabolism
[edit]Low ATP in skeletal muscle
[edit]Patients with fibromyalgia experience exercise intolerance. Primary fibromyalgia is idiopathic (cause unknown), whereas secondary fibromyalgia is in association with a known underlying disorder (such as Ankylosing spondylitis).[110][non-primary source needed] In patients with primary fibromyalgia, studies have found disruptions in energy metabolism within skeletal muscle, including: decreased levels of ATP, ADP, and phosphocreatine, and increased levels of AMP and creatine (use of creatine kinase and myokinase in the phosphagen system due to low ATP);[111][non-primary source needed] increased pyruvate;[112][non-primary source needed] as well as reduced capillary density impairing oxygen delivery to the muscle cells for oxidative phosphorylation.[113][114][non-primary source needed]
Low ATP in brain
[edit]Despite being a small percentage of the body's total mass, the brain consumes approximately 20% of the energy produced by the body.[76][non-primary source needed] Parts of the brain—the anterior cingulate cortex (ACC), thalamus, and insula—were studied using proton magnetic resonance spectroscopy (MRS) in patients with fibromyalgia and compared to healthy controls. The fibromyalgia patients were found to have lower phosphocreatine (PCr) and lower creatine (Cr) than the control group. Phosphocreatine is used in the phosphagen system to produce ATP. The study found that low creatine and low phosphocreatine were associated with high pain, and that high stress, including PTSD, may contribute to these low levels.[76][non-primary source needed]
Low phosphocreatine levels may disrupt glutamate neurotransmission within the brains of those with fibromyalgia. Glutamate/creatine ratios within the bilateral ventrolateral prefrontal cortex were found to be significantly higher than in controls.[76][96][non-primary source needed]
Diagnosis
[edit]
There is no single pathological feature, laboratory finding, or biomarker that can diagnose fibromyalgia and there is debate over what should be considered diagnostic criteria and whether an objective diagnosis is possible.[80] In most cases, people with fibromyalgia symptoms may have laboratory test results that appear normal and many of their symptoms may mimic those of other rheumatic conditions such as arthritis or osteoporosis. The specific diagnostic criteria for fibromyalgia have evolved over time.[115]
American College of Rheumatology
[edit]The first widely accepted set of classification criteria for research purposes was elaborated in 1990 by the Multicenter Criteria Committee of the American College of Rheumatology. These criteria, which are known informally as "the ACR 1990", defined fibromyalgia according to the presence of the following criteria:
- A history of widespread pain lasting more than three months – affecting all four quadrants of the body, i.e., both sides, and above and below the waist.
- Tender points – there are 18 designated possible tender points (although a person with the disorder may feel pain in other areas as well).
The ACR criteria for the classification of patients were originally established as inclusion criteria for research purposes and were not intended for clinical diagnosis but have later become the de facto diagnostic criteria in the clinical setting. A controversial study was done by a legal team looking to prove their client's disability based primarily on tender points and their widespread presence in non-litigious communities prompted the lead author of the ACR criteria to question now the useful validity of tender points in diagnosis.[116] Use of control points has been used to cast doubt on whether a person has fibromyalgia, and to claim the person is malingering.[22]

In 2010, the American College of Rheumatology approved provisional revised diagnostic criteria for fibromyalgia that eliminated the 1990 criteria's reliance on tender point testing.[34] The revised criteria used a widespread pain index (WPI) and symptom severity scale (SSS) in place of tender point testing under the 1990 criteria. The WPI counts up to 19 general body areas[a] in which the person has experienced pain in the preceding week.[9] The SSS rates the severity of the person's fatigue, unrefreshed waking, cognitive symptoms, and general somatic symptoms,[b] each on a scale from 0 to 3, for a composite score ranging from 0 to 12.[9] The revised criteria for diagnosis were:
- WPI ≥ 7 and SSS ≥ 5 OR WPI 3–6 and SSS ≥ 9,
- Symptoms have been present at a similar level for at least three months, and
- No other diagnosable disorder otherwise explains the pain.[34]: 607
In 2016, the provisional criteria of the American College of Rheumatology from 2010 were revised.[9] The new diagnosis required all of the following criteria:
- "Generalized pain, defined as pain in at least 4 of 5 regions, is present."
- "Symptoms have been present at a similar level for at least 3 months."
- "Widespread pain index (WPI) ≥ 7 and symptom severity scale (SSS) score ≥ 5 OR WPI of 4–6 and SSS score ≥ 9."
- "A diagnosis of fibromyalgia is valid irrespective of other diagnoses. A diagnosis of fibromyalgia does not exclude the presence of other clinically important illnesses."[9]
American Pain Society 2019
[edit]In 2019, the American Pain Society in collaboration with the U.S. Food and Drug Administration developed a new diagnostic system using two dimensions.[12] The first dimension included core diagnostic criteria and the second included common features. In accordance to the 2016 diagnosis guidelines, the presence of another medical condition or pain disorder does not rule out the diagnosis of fibromyalgia. Nonetheless, other conditions should be ruled out as the main explaining reason for the patient's symptoms. The core diagnostic criteria are:[117]
- Multisite pain defined as six or more pain sites from a total of nine possible sites (head, arms, chest, abdomen, upper back, lower back, and legs), for at least three months
- Moderate to severe sleep problems or fatigue, for at least three months
Common features found in fibromyalgia patients can assist the diagnosis process. These are tenderness (sensitivity to light pressure), dyscognition (difficulty to think), musculoskeletal stiffness, and environmental sensitivity or hypervigilance.[12]
Self-report questionnaires
[edit]Some research has suggested using a multidimensional approach taking into consideration somatic symptoms, psychological factors, psychosocial stressors and subjective belief regarding fibromyalgia.[118] These symptoms can be assessed by several self-report questionnaires.[9]
Widespread Pain Index (WPI)
[edit]The Widespread Pain Index (WPI) was introduced by the American College of Rheumatology in 2010. It measures the number of painful body regions.[34] The revised criteria counts up to 19 general body areas: shoulder girdle, upper arm, lower arm, hip/buttock/trochanter, upper leg, lower leg, jaw, all left & right; plus the chest, abdomen, neck and upper and lower back.[34] The 2016 ACR criteria required a Widespread pain index (WPI) ≥ 7 or WPI of 4–6 for higher severity pain.
Symptom Severity Scale (SSS)
[edit]The Symptom Severity Scale (SSS) assesses the severity of the fibromyalgia symptoms.
Fibromyalgia Impact Questionnaire (FIQ)
[edit]The Fibromyalgia Impact Questionnaire (FIQ)[119] and the Revised Fibromyalgia Impact Questionnaire (FIQR)[120] assess three domains: function, overall impact and symptoms.[120] It is considered a useful measure of disease impact.[121]
Other questionnaires
[edit]Other measures include the Hospital Anxiety and Depression Scale, Multiple Ability Self-Report Questionnaire,[122] Multidimensional Fatigue Inventory, and Medical Outcomes Study Sleep Scale.
Differential diagnosis
[edit]As of 2009, as many as two out of every three people who are told that they have fibromyalgia by a rheumatologist may have some other medical condition instead.[123] Fibromyalgia could be misdiagnosed in cases of early undiagnosed rheumatic diseases such as preclinical rheumatoid arthritis, early stages of inflammatory spondyloarthritis, polymyalgia rheumatica, myofascial pain syndromes and hypermobility syndrome.[11][124] Neurological diseases with an important pain component include multiple sclerosis, Parkinson's disease and peripheral neuropathy.[11][124] Other medical illnesses that should be ruled out are endocrine disease or metabolic disorder (hypothyroidism, hyperparathyroidism, acromegaly, vitamin D deficiency), gastro-intestinal disease (celiac and non-celiac gluten sensitivity), infectious diseases (Lyme disease, hepatitis C and immunodeficiency disease) and the early stages of a malignancy such as multiple myeloma, metastatic cancer and leukemia/lymphoma.[11][124] Other systemic, inflammatory, endocrine, rheumatic, infectious, and neurologic disorders may cause fibromyalgia-like symptoms, such as systemic lupus erythematosus, Sjögren syndrome, ankylosing spondylitis, Ehlers-Danlos syndromes, psoriatic-related polyenthesitis, a nerve compression syndrome (such as carpal tunnel syndrome), and myasthenia gravis.[125][123][126][127] In addition, several medications can also evoke pain (statins, aromatase inhibitors, bisphosphonates, and opioids).[12]
The differential diagnosis is made during the evaluation on the basis of the person's medical history, physical examination, and laboratory investigations.[125][123][126][127] The patient's history can provide some hints to a fibromyalgia diagnosis. A family history of early chronic pain, a childhood history of pain, an emergence of broad pain following physical and/or psychosocial stress, a general hypersensitivity to touch, smell, noise, taste, hypervigilance, and various somatic symptoms (gastrointestinal, urology, gynecology, neurology), are all examples of these signals.[11]
Extensive laboratory tests are usually unnecessary in the differential diagnosis of fibromyalgia.[12] Common tests that are conducted include complete blood count, comprehensive metabolic panel, erythrocyte sedimentation rate, C-reactive protein, and thyroid function test.[12]
Management
[edit]Universally accepted treatments typically consist of symptom management and improving patient quality of life.[16] A personalized, multidisciplinary approach to treatment that includes pharmacologic considerations and begins with effective patient education is most beneficial.[16] Developments in the understanding of the pathophysiology of the disorder have led to improvements in treatment, which include prescription medication, behavioral intervention, and exercise.
A number of associations have published guidelines for the diagnosis and management of fibromyalgia. The European League Against Rheumatism (EULAR; 2017)[17] recommends a multidisciplinary approach, allowing a quick diagnosis and patient education. The recommended initial management should be non-pharmacological, later pharmacological treatment can be added. The European League Against Rheumatism gave the strongest recommendation for aerobic and strengthening exercise. Weak recommendations were given to a number of treatments, based on their outcomes. Qigong, yoga, and tai chi were weakly recommended for improving sleep and quality of life. Mindfulness was weakly recommended for improving pain and quality of life. Acupuncture and hydrotherapy were weakly recommended for improving pain. A weak recommendation was also given to psychotherapy. It was more suitable for patients with mood disorders or unhelpful coping strategies. Chiropractic was strongly recommended against, due to safety concerns. Some medications were weakly recommended for severe pain (duloxetine, pregabalin, tramadol) or sleep disturbance (amitriptyline, cyclobenzaprine, pregabalin). Others were not recommended due to a lack of efficacy (nonsteroidal anti-inflammatory drugs, monoamine oxidase inhibitors and selective serotonin reuptake inhibitors). Growth hormone, sodium oxybate, opioids and steroids were strongly recommended against due to lack of efficacy and side effects.
The guidelines published by the Association of the Scientific Medical Societies in Germany[128] inform patients that self-management strategies are an important component in managing the disease.[129] The Canadian Pain Society[130] also published guidelines for the diagnosis and management of fibromyalgia.
Exercise
[edit]Exercise is the only fibromyalgia treatment that has been given a strong recommendation by the European Alliance of Associations for Rheumatology (EULAR). There is strong evidence indicating that exercise improves fitness, sleep and quality of life and may reduce pain and fatigue for people with fibromyalgia.[131][21][132] Exercise has an added benefit in that it does not cause any serious adverse effects.[132] There are a number of hypothesized biological mechanisms.[133] Exercise may improve pain modulation[134][135] through serotoninergic pathways.[135] It may reduce pain by altering the hypothalamic-pituitary-adrenal axis and reducing cortisol levels.[136] It also has anti-inflammatory effects that may improve fibromyalgia symptoms.[137][138] Aerobic exercise can improve muscle metabolism and pain through mitochondrial pathways.[137]
When different exercise programs are compared, aerobic exercise is capable of modulating the autonomic nervous function of fibromyalgia patients, whereas resistance exercise does not show such effects.[139] A 2022 meta-analysis found that aerobic training showed a high effect size while strength interventions showed moderate effects.[140] Meditative exercise seems preferable for improving sleep,[141][142] with no differences between resistance, flexibility and aquatic exercise in their favorable effects on fatigue.[141]
Despite its benefits, exercise is a challenge for patients with fibromyalgia, due to the chronic fatigue and pain they experience.[143] They may also feel that those who recommend or deliver exercise interventions do not fully understand the possible negative impact of exercise on fatigue and pain.[144] This is especially true for non-personalized exercise programs.[144] Adherence is higher when the exercise program is recommended by doctors or supervised by nurses.[145]
Sufferers perceive exercise as more effortful than healthy adults.[146] Depression and higher pain intensity serve as barriers to physical activity.[147] Exercise may intimidate them, in fear that they will be asked to do more than they are capable of.[144]
A recommended approach to a graded exercise program begins with small, frequent exercise periods and builds up from there.[140][148] In order to reduce pain the use of an exercise program of 13 to 24 weeks is recommended, with each session lasting 30 to 60 minutes.[140]
Aerobic
[edit]Aerobic exercise for fibromyalgia patients is the most investigated type of exercise.[132] It includes activities such as walking, jogging, spinning, cycling, dancing and exercising in water,[137][139] with walking being named as one of the best methods.[149] A 2017 Cochrane summary concluded that aerobic exercise probably improves quality of life, slightly decreases pain and improves physical function and makes no difference in fatigue and stiffness.[150] A 2019 meta-analysis showed that exercising aerobically can reduce autonomic dysfunction and increase heart rate variability.[139] This happens when patients exercise at least twice a week, for 45–60 minutes at about 60%-80% of the maximum heart rate.[139] Aerobic exercise also decreases anxiety and depression and improves the quality of life.[139]
Flexibility
[edit]Combinations of different exercises such as flexibility and aerobic training may improve stiffness.[151] However, the evidence is of low-quality.[151] It is not clear if flexibility training alone compared to aerobic training is effective at reducing symptoms or has any adverse effects.[152]
Resistance
[edit]In resistance exercise, participants apply a load to their body using weights, elastic band, body weight or other measures.
Two meta-analyses on fibromyalgia have shown that resistance training can reduce anxiety and depression,[139][153] one found that it decreases pain and disease severity[154] and one found that it improves quality of life.[139] Resistance training may also improve sleep, with a greater effect than that of flexibility training and a similar effect to that of aerobic exercise.[155]
The dosage of resistance exercise for women with fibromyalgia was studied in a 2022 meta-analysis.[156] Effective dosages were found when exercising twice a week, for at least eight weeks. Symptom improvement was found for even low dosages such as 1–2 sets of 4–20 repetitions.[156] Most studies use moderate exercise intensity of 40% to 85% one-repetition maximum. This intensity was effective in reducing pain.[156] Some treatment regimes increase the intensity over time (from 40% to 80%), whereas others increase it when the participant is able to perform 12 repetitions.[156] High-intensity exercises may cause lower treatment adherence.
Meditative
[edit]A 2021 meta-analysis found that meditative exercise programs (tai chi, yoga, qigong) were superior to other forms of exercise (aerobic, flexibility, resistance) in improving sleep quality.[141] Other meta-analyses also found positive effects of tai chi for sleep,[157] fibromyalgia symptoms,[158] and pain, fatigue, depression and quality of life.[159] These tai chi interventions frequently included 1-hour sessions practiced 1-3 times a week for 12 weeks. Meditative exercises, as a whole, may achieve desired outcomes through biological mechanisms such as antioxidation, anti-inflammation, reduction in sympathetic activity and modulation of glucocorticoid receptor sensitivity.[137]
Aquatic
[edit]Several reviews and meta-analyses suggest that aquatic training can improve symptoms and wellness in people with fibromyalgia.[160][161][162][163][164][165] It is recommended to practice aquatic therapy at least twice a week using a low to moderate intensity.[164] However, aquatic therapy does not appear to be superior to other types of exercise.[166]
Other
[edit]Limited evidence suggests vibration training in combination with exercise may improve pain, fatigue, and stiffness.[167]
Medications
[edit]A few countries have published guidelines for the management and treatment of fibromyalgia. As of 2018, all of them emphasize that medications are not required. However, medications, though imperfect, continue to be a component of treatment strategy for fibromyalgia patients. The German guidelines outlined parameters for drug therapy termination and recommended considering drug holidays after six months.[18]
Health Canada and the US Food and Drug Administration (FDA) have approved pregabalin[168] (an anticonvulsant) and duloxetine (a serotonin–norepinephrine reuptake inhibitor) for the management of fibromyalgia. The FDA also approved milnacipran (another serotonin–norepinephrine reuptake inhibitor), but the European Medicines Agency refused marketing authority.[169]
The medications duloxetine, milnacipran, or pregabalin have been approved by the US Food and Drug Administration (FDA) for the management of fibromyalgia.[170]
Antidepressants
[edit]Antidepressants are one of the common drugs for fibromyalgia. A 2021 meta-analysis concluded that antidepressants can improve the quality of life for fibromyalgia patients in the medium-term.[19] For most people with fibromyalgia, the potential benefits of treatment with the serotonin and norepinephrine reuptake inhibitors duloxetine and milnacipran and the tricyclic antidepressants, such as amitriptyline, are outweighed by significant adverse effects (more adverse effects than benefits), however, a small number of people may experience relief from symptoms with these medications.[171][172][173]
The length of time that antidepressant medications take to be effective at reducing symptoms can vary. Any potential benefits from the antidepressant amitriptyline may take up to three months to take effect and it may take between three and six months for duloxetine, milnacipran, and pregabalin to be effective at improving symptoms.[174] Some medications have the potential to cause withdrawal symptoms when stopping so gradual discontinuation may be warranted particularly for antidepressants and pregabalin.[22]
Serotonin and norepinephrine reuptake inhibitors
[edit]A 2023 meta analysis found that duloxetine improved fibromyalgia symptoms, regardless of the dosage.[175] SSRIs may be also be used to treat depression in people diagnosed with fibromyalgia.[176]
Tricyclic antidepressants
[edit]While amitriptyline has been used as a first line treatment, the quality of evidence to support this use and comparison between different medications is poor.[177][173] Very weak evidence indicates that a very small number of people may benefit from treatment with the tetracyclic antidepressant mirtazapine, however, for most, the potential benefits are not great and the risk of adverse effects and potential harm outweighs any potential for benefit.[178] As of 2018, the only tricyclic antidepressant that has sufficient evidence is amitriptyline.[18][177]
Monoamine oxidase inhibitors
[edit]Tentative evidence suggests that monoamine oxidase inhibitors (MAOIs) such as pirlindole and moclobemide are moderately effective for reducing pain.[179] Very low-quality evidence suggests pirlindole as more effective at treating pain than moclobemide.[179] Side effects of MAOIs may include nausea and vomiting.[179]
Central nervous system depressants
[edit]Central nervous system depressants include drug categories such as sedatives, tranquilizers, and hypnotics. A 2021 meta-analysis concluded that such drugs can improve the quality of life for fibromyalgia patients in the medium-term.[19]
Anti-seizure medication
[edit]The anti-convulsant medications gabapentin and pregabalin may be used to reduce pain.[8] There is tentative evidence that gabapentin may be of benefit for pain in about 18% of people with fibromyalgia.[8] It is not possible to predict who will benefit, and a short trial may be recommended to test the effectiveness of this type of medication. Approximately 6/10 people who take gabapentin to treat pain related to fibromyalgia experience unpleasant side effects such as dizziness, abnormal walking, or swelling from fluid accumulation.[180] Pregabalin demonstrates a benefit in about 9% of people.[181] Pregabalin reduced time off work by 0.2 days per week.[182]
Cannabinoids
[edit]Cannabinoids may have some benefits for people with fibromyalgia. However, as of 2022, the data on the topic is still limited.[183][184][185] Cannabinoids may also have adverse effects and may negatively interact with common rheumatological drugs.[186]
Opioids
[edit]The use of opioids is controversial. As of 2015, no opioid is approved for use in this condition by the FDA.[187] A 2016 Cochrane review concluded that there is no good evidence to support or refute the suggestion that oxycodone, alone or in combination with naloxone, reduces pain in fibromyalgia.[188] The National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) in 2014 stated that there was a lack of evidence for opioids for most people.[5] The Association of the Scientific Medical Societies in Germany in 2012 made no recommendation either for or against the use of weak opioids because of the limited amount of scientific research addressing their use in the treatment of fibromyalgia. They strongly advise against using strong opioids.[128] The Canadian Pain Society in 2012 said that opioids, starting with a weak opioid like tramadol, can be tried but only for people with moderate to severe pain that is not well-controlled by non-opioid painkillers. They discourage the use of strong opioids and only recommend using them while they continue to provide improved pain and functioning. Healthcare providers should monitor people on opioids for ongoing effectiveness, side effects, and possible unwanted drug behaviors.[130]
A 2015 review found fair evidence to support tramadol use if other medications do not work.[187] A 2018 review found little evidence to support the combination of paracetamol (acetaminophen) and tramadol over a single medication.[189] Goldenberg et al suggest that tramadol works via its serotonin and norepinephrine reuptake inhibition, rather than via its action as a weak opioid receptor agonist.[190]
A large study of US people with fibromyalgia found that between 2005 and 2007 37.4% were prescribed short-acting opioids and 8.3% were prescribed long-acting opioids,[3] with around 10% of those prescribed short-acting opioids using tramadol;[191] and a 2011 Canadian study of 457 people with fibromyalgia found 32% used opioids and two-thirds of those used strong opioids.[130]
Topical treatment
[edit]Capsaicin has been suggested as a topical pain reliever. Preliminary results suggest that it may improve sleep quality and fatigue, but there are not enough studies to support this claim.[192]
Unapproved or unfounded
[edit]Sodium oxybate increases growth hormone production levels through increased slow-wave sleep patterns. However, this medication was not approved by the FDA for the indication for use in people with fibromyalgia due to the concern for abuse.[193]
The muscle relaxants cyclobenzaprine, carisoprodol with acetaminophen and caffeine, and tizanidine are sometimes used to treat fibromyalgia; however, as of 2015 they are not approved for this use in the United States.[194][195] The use of nonsteroidal anti-inflammatory drugs is not recommended as first-line therapy.[196] Moreover, nonsteroidal anti-inflammatory drugs cannot be considered as useful in the management of fibromyalgia.[197]
Very low-quality evidence suggests quetiapine may be effective in fibromyalgia.[198]
No high-quality evidence exists that suggests synthetic THC (nabilone) helps with fibromyalgia.[199]
Nutrition and dietary supplements
[edit]Nutrition is related to fibromyalgia in several ways. Some nutritional risk factors for fibromyalgia complications are obesity, nutritional deficiencies, food allergies and consuming food additives.[200] The consumption of fruits and vegetables, low-processed foods, high-quality proteins, and healthy fats may have some benefits.[200] Low-quality evidence found some benefits of a vegetarian or vegan diet.[201]
Although dietary supplements have been widely investigated in relation to fibromyalgia, most of the evidence, as of 2021, is of poor quality. It is therefore difficult to reach conclusive recommendations.[202] It appears that Q10 coenzyme and vitamin D supplements can reduce pain and improve quality of life for fibromyalgia patients.[21][203] Q10 coenzyme has beneficial effects on fatigue in fibromyalgia patients, with most studies using doses of 300 mg per day for three months.[204] Q10 coenzyme is hypothesized to improve mitochondrial activity and decrease inflammation.[205] Vitamin D has been shown to improve some fibromyalgia measures, but not others.[203][206]
Two review articles found that melatonin treatment has several positive effects on fibromyalgia patients, including the improvement of sleep quality, pain, and disease impact.[207][208] No major adverse events were reported.[207]
Psychotherapy
[edit]Due to the uncertainty about the pathogenesis of fibromyalgia, current treatment approaches focus on management of symptoms to improve quality of life,[209] using integrated pharmacological and non-pharmacological approaches.[4] There is no single intervention shown to be effective for all patients.[210] In a 2020 Cochrane review, cognitive behavioral therapy was found to have a small but beneficial effect for reducing pain and distress but adverse events were not well evaluated.[211] Cognitive behavioral therapy and related psychological and behavioural therapies have a small to moderate effect in reducing symptoms of fibromyalgia.[212][213] Effect sizes tend to be small when cognitive behavioral therapy is used as a stand-alone treatment for patients with fibromyalgia, but these improve significantly when it is part of a wider multidisciplinary treatment program.[213]
A 2010 systematic review of 14 studies reported that cognitive behavioral therapy improves self-efficacy or coping with pain and reduces the number of physician visits at post-treatment, but has no significant effect on pain, fatigue, sleep, or health-related quality of life at post-treatment or follow-up. Depressed mood was also improved but this could not be distinguished from some risks of bias.[214] A 2022 meta-analysis found that cognitive behavioral therapy reduces insomnia in people with chronic pain, including people with fibromyalgia.[215] Acceptance and commitment therapy, a type of cognitive behavioral therapy, has also proven effective.[216]
Patient education
[edit]Patient education is recommended by the European League Against Rheumatism (EULAR) as an important treatment component.[17] As of 2022, there is only low-quality evidence showing that patient education can decrease pain and fibromyalgia impact.[217][218]
Sleep hygiene interventions show low effectiveness in improving insomnia in people with chronic pain.[215]
Physical therapy
[edit]Patients with chronic pain, including those with fibromyalgia, can benefit from techniques such as manual therapy, cryotherapy, and balneotherapy.[219] These can lessen the experience of chronic pain and increase both the amount and quality of sleep. Patients' quality of life is also improved by decreasing pain mechanisms and increasing sleep quality, particularly during the REM phase, sleep efficiency, and alertness.[219]
Manual therapy
[edit]A 2021 meta-analysis concluded that massage and myofascial release diminish pain in the medium-term.[19] As of 2015, there was no good evidence for the benefit of other mind-body therapies.[220]
Acupuncture
[edit]A 2013 review found moderate-level evidence on the usage of acupuncture with electrical stimulation for improvement of the overall well-being. Acupuncture alone will not have the same effects, but will enhance the influence of exercise and medication in pain and stiffness.[221]
Electrical neuromodulation
[edit]Several forms of electrical neuromodulation, including transcutaneous electrical nerve stimulation (TENS) and transcranial direct current stimulation (tDCS), have been used to treat fibromyalgia. In general, they have been found to be helpful in reducing pain and depression and improving functioning.[222][223]
Transcutaneous electrical nerve stimulation (TENS)
[edit]Transcutaneous electrical nerve stimulation (TENS) is the delivery of pulsed electrical currents to the skin to stimulate peripheral nerves. TENS is widely used to treat pain and is considered to be a low-cost, safe, and self-administered treatment.[224] As such, it is commonly recommended by clinicians to people suffering from pain.[225] On 2019, an overview of eight Cochrane reviews was conducted, covering 51 TENS-related randomized controlled trials.[225] The review concluded that the quality of the available evidence was insufficient to make any recommendations.[225] A later review concluded that transcutaneous electrical nerve stimulation may diminish pain in the short-term, but there was uncertainty about the relevance of the results.[19]
Preliminary findings suggest that electrically stimulating the vagus nerve through an implanted device can potentially reduce fibromyalgia symptoms.[226] However, there may be adverse reactions to the procedure.[226]
Noninvasive brain stimulation
[edit]Noninvasive brain stimulation includes methods such as transcranial direct current stimulation and high-frequency repetitive transcranial magnetic stimulation (TMS). Both methods have been found to improve pain scores in neuropathic pain and fibromyalgia.[227]
A 2023 meta analysis of 16 RCTs found that transcranial direct current stimulation (tDCS) of over 4 weeks can decrease pain in patients with fibromyalgia.[228]
A 2021 meta-analysis of multiple intervention types concluded that magnetic field therapy and transcranial magnetic stimulation may diminish pain in the short-term, but conveyed an uncertainty about the relevance of the result.[19] Several 2022 meta-analyses focusing on transcranial magnetic stimulation found positive effects on fibromyalgia.[229][230][231] Repetitive transcranial magnetic stimulation improved pain in the short-term[230][231] and quality of life after 5–12 weeks.[230][231] Repetitive transcranial magnetic stimulation did not improve anxiety, depression, and fatigue.[231] Transcranial magnetic stimulation to the left dorsolateral prefrontal cortex was also ineffective.[230]
EEG neurofeedback
[edit]A systematic review of EEG neurofeedback for treatment of fibromyalgia found most treatments showed significant improvements of the main symptoms of the disease.[232] However, the protocols were so different, and the lack of controls or randomization impede drawing conclusive results.[232]
Hyperbaric oxygen therapy
[edit]Hyperbaric oxygen therapy (HBOT) has shown beneficial effects in treating chronic pain by reducing inflammation and oxidative stress.[99] However, treating fibromyalgia with hyperbaric oxygen therapy is still controversial, in light of the scarcity of large-scale clinical trials.[137] In addition, hyperbaric oxygen therapy raises safety concerns due to the oxidative damage that may follow it.[137] An evaluation of nine trials with 288 patients in total found that HBOT was more effective at relieving fibromyalgia patients' pain than the control intervention. In most of the trials HBOT improved sleep disturbance, multidimensional function, patient satisfaction, and tender spots. 24% of the patients experienced negative outcomes.[233]
Prognosis
[edit]Although in itself fibromyalgia is neither degenerative nor fatal, the chronic pain of fibromyalgia is pervasive and persistent. Most people with fibromyalgia report that their symptoms do not improve over time. However, most patients learn to adapt to the symptoms over time. The German guidelines for patients explain that:
- The symptoms of fibromyalgia are persistent in nearly all patients.
- Total relief of symptoms is seldom achieved.
- The symptoms do not lead to disablement and do not shorten life expectancy.[129]
An 11-year follow-up study on 1,555 patients found that most remained with high levels of self-reported symptoms and distress.[non-primary source needed][234] However, there was a great deal of patient heterogeneity accounting for almost half of the variance. At the final observation, 10% of the patients showed substantial improvement with minimal symptoms. An additional 15% had moderate improvement. This state, though, may be transient, given the fluctuations in symptom severity.[non-primary source needed][234]
A study of 97 adolescents diagnosed with fibromyalgia followed them for eight years.[non-primary source needed] After eight years, the majority of youth still experienced pain and disability in physical, social, and psychological areas. At the last follow-up, all participants reported experiencing one or more fibromyalgia symptoms such as pain, fatigue, and/or sleep problems, with 58% matching the complete ACR 2010 criteria for fibromyalgia. Based on the WPI and SS score cut-points, the remaining 42% exhibited subclinical symptoms. Pain and emotional symptom trajectories, on the other hand, displayed a variety of longitudinal patterns. The study concluded that while most patient's fibromyalgia symptoms endure, the severity of their pain tends to reduce over time.[235]
Baseline depressive symptoms in adolescents appear to predict worse pain at follow-up periods.[236][237]
A meta-analysis based on close to 200,000 fibromyalgia patients found that they were at a higher risk for all-cause mortality. Specific mortality causes that were suggested were accidents, infections and suicide.[238]
Epidemiology
[edit]Fibromyalgia is estimated to affect 1.8% of the population.[239]
Despite the fact that more than 90% of fibromyalgia patients are women, only 60% of people with fibromyalgia symptoms are female in the general population.[240]
Society and culture
[edit]Economics
[edit]People with fibromyalgia generally have higher healthcare costs and utilization rates. A review of 36 studies found that fibromyalgia causes a significant economic burden on health care systems.[241] Annual costs per patient were estimated to be up to $35,920 in the US and $8,504 in Europe.[241]
Controversies
[edit]Fibromyalgia was defined relatively recently. In the past, it was a disputed diagnosis. Rheumatologist, Frederick Wolfe, lead author of the 1990 paper that first defined the diagnostic guidelines for fibromyalgia, stated in 2008 that he believed it "clearly" not to be a disease but instead a physical response to depression and stress.[242] In 2013, Wolfe added that its causes "are controversial in a sense" and "there are many factors that produce these symptoms – some are psychological and some are physical and it does exist on a continuum".[243] Some members of the medical community do not consider fibromyalgia a disease because of a lack of abnormalities on physical examination and the absence of objective diagnostic tests.[28][244]
In the past, some psychiatrists have viewed fibromyalgia as a type of affective disorder, or a somatic symptom disorder. These controversies do not engage healthcare specialists alone; some patients object to fibromyalgia being described in purely somatic terms.[245]
As of 2022, neurologists and pain specialists tend to view fibromyalgia as a pathology due to dysfunction of muscles and connective tissue as well as functional abnormalities in the central nervous system. Rheumatologists define the syndrome in the context of "central sensitization" – heightened brain response to normal stimuli in the absence of disorders of the muscles, joints, or connective tissues. Because of this symptomatic overlap, some researchers have proposed that fibromyalgia and other analogous syndromes be classified together as central sensitivity syndromes.[246][13]
Notes
[edit]- ^ Shoulder girdle (left & right), upper arm (left & right), lower arm (left & right), hip/buttock/trochanter (left & right), upper leg (left & right), lower leg (left & right), jaw (left & right), chest, abdomen, back (upper & lower), and neck.[34]: 607
- ^ Somatic symptoms include, but are not limited to: muscle pain, irritable bowel syndrome, fatigue or tiredness, problems thinking or remembering, muscle weakness, headache, pain or cramps in the abdomen, numbness or tingling, dizziness, insomnia, depression, constipation, pain in the upper abdomen, nausea, nervousness, chest pain, blurred vision, fever, diarrhea, dry mouth, itching, wheezing, Raynaud's phenomenon, hives or welts, ringing in the ears, vomiting, heartburn, oral ulcers, loss of or changes in taste, seizures, dry eyes, shortness of breath, loss of appetite, rash, sun sensitivity, hearing difficulties, easy bruising, hair loss, frequent or painful urination, and bladder spasms.[34]: 607
References
[edit]- ^ "fibromyalgia". Collins Dictionaries. Archived from the original on 4 October 2015. Retrieved 16 March 2016.
- ^ "Neurology Now: Fibromyalgia: Is Fibromyalgia Real? | American Academy of Neurology". tools.aan.com. October 2009. Retrieved 1 June 2018.[permanent dead link]
- ^ Jump up to: a b c Ngian GS, Guymer EK, Littlejohn GO (February 2011). "The use of opioids in fibromyalgia". International Journal of Rheumatic Diseases. 14 (1): 6–11. doi:10.1111/j.1756-185X.2010.01567.x. PMID 21303476. S2CID 29000267.
- ^ Jump up to: a b c d e f g h i j k l Clauw DJ (April 2014). "Fibromyalgia: a clinical review". JAMA. 311 (15): 1547–1555. doi:10.1001/jama.2014.3266. PMID 24737367. S2CID 43693607.
- ^ Jump up to: a b c d e f g "Questions and Answers about Fibromyalgia". NIAMS. July 2014. Archived from the original on 15 March 2016. Retrieved 15 March 2016.
- ^ Ferri FF (2010). "Chapter F". Ferri's differential diagnosis: a practical guide to the differential diagnosis of symptoms, signs, and clinical disorders (2nd ed.). Philadelphia, PA: Elsevier/Mosby. ISBN 978-0-323-07699-9.
- ^ Schneider MJ, Brady DM, Perle SM (2006). "Commentary: differential diagnosis of fibromyalgia syndrome: proposal of a model and algorithm for patients presenting with the primary symptom of chronic widespread pain". Journal of Manipulative and Physiological Therapeutics. 29 (6): 493–501. doi:10.1016/j.jmpt.2006.06.010. PMID 16904498.
- ^ Jump up to: a b c Cooper TE, Derry S, Wiffen PJ, Moore RA (January 2017). "Gabapentin for fibromyalgia pain in adults". The Cochrane Database of Systematic Reviews. 1 (1): CD012188. doi:10.1002/14651858.CD012188.pub2. PMC 6465053. PMID 28045473.
- ^ Jump up to: a b c d e f g h Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Häuser W, Katz RL, et al. (December 2016). "2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria". Seminars in Arthritis and Rheumatism. 46 (3): 319–329. doi:10.1016/j.semarthrit.2016.08.012. PMID 27916278.
- ^ Jump up to: a b Wu YL, Chang LY, Lee HC, Fang SC, Tsai PS (May 2017). "Sleep disturbances in fibromyalgia: A meta-analysis of case-control studies". Journal of Psychosomatic Research. 96: 89–97. doi:10.1016/j.jpsychores.2017.03.011. PMID 28545798.
- ^ Jump up to: a b c d e f g Häuser W, Sarzi-Puttini P, Fitzcharles MA (2019). "Fibromyalgia syndrome: under-, over- and misdiagnosis". Clinical and Experimental Rheumatology. 37 (1 Suppl 116): 90–97. PMID 30747096.
- ^ Jump up to: a b c d e f g h i j k l m n o p q r s t u Arnold LM, Bennett RM, Crofford LJ, Dean LE, Clauw DJ, Goldenberg DL, et al. (June 2019). "AAPT Diagnostic Criteria for Fibromyalgia". The Journal of Pain. 20 (6): 611–628. doi:10.1016/j.jpain.2018.10.008. hdl:2434/632765. PMID 30453109. S2CID 53872511.
- ^ Jump up to: a b c Mezhov V, Guymer E, Littlejohn G (December 2021). "Central sensitivity and fibromyalgia". Internal Medicine Journal. 51 (12): 1990–1998. doi:10.1111/imj.15430. PMID 34139045. S2CID 235471910.
- ^ Bergmann U (2012). Neurobiological foundations for EMDR practice. New York: Springer Pub. Co. p. 165. ISBN 978-0-8261-0938-5.
- ^ Jump up to: a b c d e f g Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W (май 2021). «Ноципластическая боль: к пониманию распространенных боли». Лансет . 397 (10289): 2098–2110. doi : 10.1016/s0140-6736 (21) 00392-5 . PMID 34062144 . S2CID 235245552 .
- ^ Jump up to: а беременный в Прабхакар А., Кайзер Дж. М., Новач М.Б., Корнетт Э.М., Урман Р.Д., Кей А.Д. (март 2019 г.). «Роль лечения дополнительной и альтернативной медицины при фибромиалгии: всесторонний обзор». Текущие ревматологические отчеты . 21 (5): 14. doi : 10.1007/s11926-019-0814-0 . PMID 30830504 . S2CID 73482737 .
- ^ Jump up to: а беременный в дюймовый и фон Macfarlane GJ, Kronisch C, Atzeni F, Häuser W, Choy EH, Amris K, et al. (Декабрь 2017). «РЕКОМЕНДАЦИИ EULACE по лечению фибромиалгии» (PDF) . Анналы ревматических заболеваний . 76 (12): E54. doi : 10.1136/annrheumdis-2017-211587 . PMID 28476880 . S2CID 26251476 . Архивировано (PDF) из оригинала 8 февраля 2023 года . Получено 4 марта 2023 года .
- ^ Jump up to: а беременный в дюймовый и Häuser W, Fitzcharles MA (март 2018 г.). «Факты и мифы, относящиеся к фибромиалгии» . Диалоги в клинической нейробиологии . 20 (1): 53–62. doi : 10.31887/dcns.2018.20.1/whauser . PMC 6016048 . PMID 29946212 .
- ^ Jump up to: а беременный в дюймовый и фон глин Маскаренхас Р.О., Соуза М.Б., Оливейра М.Х., Лакерда А.С., Мендон В.А., Хеншке Н., Оливейра В.К. (январь 2021 г.). «Ассоциация терапии с пониженной болью и улучшенным качеством жизни у пациентов с фибромиалгией: систематический обзор и метаанализ» . Джама внутренняя медицина . 181 (1): 104–112. doi : 10.1001/jamainternmed.2020.5651 . PMC 7589080 . PMID 33104162 .
- ^ Kia S, Choy E (май 2017 г.). «Обновление руководства по лечению при синдроме фибромиалгии с акцентом на фармакологию» . Биомедицины . 5 (2): 20. doi : 10.3390/biomedicines5020020 . PMC 5489806 . PMID 28536363 .
- ^ Jump up to: а беременный в Ibanñez-vera aj, «Физическая терапевтическая приправы и добавки к рисованию фибромиалгии. Примечания. спорта Медицина 53 (197): 33–41. два 10.1016/j.apunts.2017.07.001:
- ^ Jump up to: а беременный в Häuser W, Eich W, Herrmann M, Utinger DO, Schiltenwolf M, Henningsen P (июнь 2009 г.). «Синдром фибромиалгии: классификация, диагностика и лечение» . Deutsches ärzteblatt International . 106 (23): 383–391. Doi : 10.3238/Доктор 2009.0383 . PMC 2712241 . PMID 19623319 .
- ^ Команда здравоохранения (февраль 2004 г.). «Фибромиалгия» . Страхование Бупа. Архивировано из оригинала 22 июня 2006 года . Получено 24 августа 2006 года .
- ^ Юнус М., Маси А.Т., Калабро Дж.Дж., Миллер К.А., Фейгенбаум С.Л. (август 1981). «Первичная фибромиалгия (фиброзит): клиническое исследование 50 пациентов с соответствующими нормальными контролями». Семинары по артриту и ревматизму . 11 (1): 151–171. doi : 10.1016/0049-0172 (81) 90096-2 . PMID 6944796 .
- ^ «Фибро-» . Dictionary.com. Архивировано из оригинала 13 декабря 2009 года . Получено 21 мая 2008 года .
- ^ "Значение мио" . 12 апреля 2009 года. Архивировано с оригинала 12 апреля 2009 года . Получено 26 августа 2012 года .
- ^ «Значение алгои» . 12 апреля 2009 года. Архивировано с оригинала 12 апреля 2009 года . Получено 26 августа 2012 года .
- ^ Jump up to: а беременный Wolfe F (апрель 2009 г.). «Фибромиалгия войн» . Журнал ревматологии . 36 (4): 671–678. doi : 10.3899/jrheum.081180 . PMID 19342721 . S2CID 2091976 .
- ^ Smythe Ha, Moldofsky H (1977). «Два вклада в понимание синдрома« фиброзита »». Бюллетень на ревматические заболевания . 28 (1): 928–931. PMID 199304 .
- ^ Уинфилд Дж.Б. (июнь 2007 г.). «Фибромиалгия и связанные с ним синдромы центральной чувствительности: двадцать пять лет прогресса». Семинары по артриту и ревматизму . 36 (6): 335–338. doi : 10.1016/j.semarthrit.2006.12.001 . PMID 17303220 .
- ^ Jump up to: а беременный Inanici F, Yunus MB (октябрь 2004 г.). «История фибромиалгии: прошлое к настоящему». Текущая боль и головная боль отчетов . 8 (5): 369–378. doi : 10.1007/s11916-996-0010-6 . PMID 15361321 . S2CID 42573740 .
- ^ Goldenberg DL (май 1987). «Синдром фибромиалгии. Новое, но противоречивое состояние». Джама . 257 (20): 2782–2787. doi : 10.1001/Jama.257.20.2782 . PMID 3553636 .
- ^ Wolfe F, Smythe Ha, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. (Февраль 1990 г.). «Американский колледж ревматологии 1990 года для классификации фибромиалгии. Отчет о многоцентровых критериях комитета». Артрит и ревматизм . 33 (2): 160–172. doi : 10.1002/art.1780330203 . PMID 2306288 .
- ^ Jump up to: а беременный в дюймовый и фон глин Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Katz RS, Mease P, et al. (Май 2010). «Предварительные диагностические критерии Американского колледжа ревматологии для фибромиалгии и измерения тяжести симптомов». Уход за артритом и исследования . 62 (5): 600–610. doi : 10.1002/acr.20140 . HDL : 2027,42/75772 . PMID 20461783 . S2CID 17154205 .
- ^ Jump up to: а беременный Clauw DJ, Arnold LM, McCarberg BH (сентябрь 2011). «Наука о фибромиалгии» . Майо -клиника . 86 (9): 907–911. doi : 10.4065/mcp.2011.0206 . PMC 3258006 . PMID 21878603 .
- ^ «ICD-11 для статистики смертности и заболеваемости» . Icd.Who.int . Архивировано с оригинала 1 августа 2018 года . Получено 9 апреля 2022 года .
- ^ Gianlorenço AC, Costa V, Fabris-Moraes W, Menacho M, Alves LG, Martinez-Magallanes D, Fregni F (15 мая 2024 г.). «Кластерный анализ при фибромиалгии: систематический обзор» . Ревматология International . doi : 10.1007/s00296-024-05616-2 . ISSN 1437-160x . PMID 38748219 .
- ^ Besiroglu MD, Dursun MD (июль 2019 г.). «Связь между фибромиалгией и женской половой дисфункцией: систематический обзор и метаанализ обсервационных исследований». Международный журнал исследований импотенции . 31 (4): 288–297. doi : 10.1038/s41443-018-0098-3 . PMID 30467351 . S2CID 53717513 .
- ^ Zdebik N, Zdebik A, Bogusławska J, Przeździecka-Dołyk J, Turn-Kręcicka A (январь 2021 г.). «Синдром фибромиалгии и глаз - обзор». Обзор офтальмологии . 66 (1): 132–137. doi : 10.1016/j.survophthal.2020.05.006 . PMID 32512032 . S2CID 219548664 .
- ^ "Архививая копия" . Academic.oup.com . Архивировано из оригинала 21 мая 2023 года . Получено 11 февраля 2024 года .
{{cite web}}: CS1 Maint: архивная копия как заголовок ( ссылка ) - ^ «Фибромиалгия - симптомы» . nhs.uk. 20 октября 2017 года. Архивировано с оригинала 23 марта 2018 года . Получено 21 октября 2020 года .
- ^ «Фибромиалгия - симптомы» . nhs.uk. 20 октября 2017 года . Получено 11 апреля 2024 года .
- ^ Кимура С., Тойора М., Тойота Й, Такаока Y (декабрь 2020 года). «Концентрации сыворотки инсулиноподобного фактора роста-1 как биомаркер улучшенного расстройства циркадного ритма сна бодрствования у детей школьного возраста» . Журнал клинического медицины сна . 16 (12): 2073–2078. doi : 10.5664/jcsm.8778 . PMC 7848940 . PMID 32876042 .
- ^ Spaeth M, Rizzi M, Sarzi-Puttini P (апрель 2011 г.). «Фибромиалгия и сон». Лучшая практика и исследования. Клиническая ревматология . 25 (2): 227–239. doi : 10.1016/j.berh.2011.03.004 . PMID 22094198 .
- ^ Jump up to: а беременный Брэдли Л.А. (декабрь 2009 г.). «Патофизиология фибромиалгии» . Американский журнал медицины . 122 (12 Suppl): S22 - S30. doi : 10.1016/j.amjmed.2009.09.008 . PMC 2821819 . PMID 19962493 .
- ^ Wolfe F, Rasker JJ, Ten Klooster P, Häuser W (декабрь 2021 г.). «Субъективная когнитивная дисфункция у пациентов с фибромиалгией и без нее: распространенность, предикторы, корреляты и последствия» . Cureus . 13 (12): E20351. doi : 10.7759/cureus.20351 . PMC 8752385 . PMID 35036191 .
- ^ Jump up to: а беременный в Bell T, Trost Z, Buelow MT, Clay O, Younger J, Moore D, Crowe M (сентябрь 2018 г.). «Мета-анализ когнитивных показателей при фибромиалгии» . Журнал клинической и экспериментальной нейропсихологии . 40 (7): 698–714. doi : 10.1080/13803395.2017.1422699 . PMC 6151134 . PMID 29388512 .
- ^ Berwick RJ, Siew S, Andersson DA, Marshall A, Goebel A (май 2021). «Систематический обзор влияния температуры на боль в фибромиалгии: метеорологические исследования и количественное сенсорное тестирование» . Журнал боли . 22 (5): 473–486. doi : 10.1016/j.jpain.2020.12.005 . PMID 33421589 . S2CID 231437516 .
- ^ Staud R, Godfrey MM, Robinson Me (август 2021 г.). «Пациенты с фибромиалгией не только гиперчувствительны к болезненным стимулам, но и к акустическим стимулам» . Журнал боли . 22 (8): 914–925. doi : 10.1016/j.jpain.2021.02.009 . PMID 33636370 . S2CID 232066286 .
- ^ Jump up to: а беременный в дюймовый и фон глин час Kleykamp BA, Ferguson MC, McNicol E, Bixho I, Arnold LM, Edwards RR, et al. (Февраль 2021 г.). «Распространенность психиатрических и хронических сопутствующих заболеваний при фибромиалгии: систематический обзор акции». Семинары по артриту и ревматизму . 51 (1): 166–174. doi : 10.1016/j.semarthrit.2020.10.006 . PMID 33383293 . S2CID 229948862 .
- ^ Habibi Asgarabad M, Salehi Yegaei P, Jafari F, Azami-Aghdash S, Lumley MA (март 2023 г.). «Отношение алекситимии с болью и другими симптомами при фибромиалгии: систематический обзор и метаанализ». Европейский журнал боли . 27 (3): 321–337. doi : 10.1002/ejp.2064 . PMID 36471652 . S2CID 254273680 .
- ^ Jump up to: а беременный в дюймовый и фон глин Fitzcharles MA, Perrot S, Häuser W (октябрь 2018 г.). «Коморбидная фибромиалгия: качественный обзор распространенности и важности» . Европейский журнал боли . 22 (9): 1565–1576. doi : 10.1002/ejp.1252 . PMID 29802812 . S2CID 44068037 .
- ^ Yepez D, Grandes Xa, Talanki Manjunatha R, Habib S, Sangaraju SL (май 2022). «Фибромиалгия и депрессия: обзор литературы их общих аспектов» . Cureus . 14 (5): E24909. doi : 10.7759/cureus.24909 . PMC 9187156 . PMID 35698706 .
- ^ Løge-Hagen JS, Sæle A, Juhl C, Bech P, Stenager E, Mellentin AI (февраль 2019 г.). «Распространенность депрессивного расстройства у пациентов с фибромиалгией: систематический обзор и метаанализ». Журнал аффективных расстройств . 245 : 1098–1105. doi : 10.1016/j.jad.2018.12.001 . PMID 30699852 . S2CID 73411416 .
- ^ Брюс Д.Ф., доктор философии. «Фибромиалгия и депрессия» . Webmd . Получено 1 апреля 2024 года .
- ^ Jump up to: а беременный Рамил-Морс Р., Берм-Бенит Е., Мартин-Мартина Л.А., Мартин-Лавин М (август 2022 г.). миталомиелитом. «Клиническое перекрытие между фибромиалгией и Отзывы . 21 : 103129 . ( 8 ) PMID 356900247 .
- ^ Jump up to: а беременный Голденберг Д.Л. (2024). «Как понять перекрытие длинного ковида, хронического синдрома усталости/миалгического энцефаломиелита, фибромиалгии и синдромов раздраженного кишечника» . Семинары по артриту и ревматизму . 67 : 152455. DOI : 10.1016/j.semarthrit.2024.152455 . PMID 38761526 .
- ^ Андерсон Г., Мэйс М (декабрь 2020 г.). «Митохондрии и иммунитет при синдроме хронической усталости». Прогресс в нейропсихофармакологии и биологической психиатрии . 103 : 109976. DOI : 10.1016/j.pnpbp.2020.109976 . PMID 32470498 . S2CID 219104988 .
- ^ Валенсия С., Фатима Х, Нванкво I, Анам М., Махарджан С., Амджад З. и др. (Октябрь 2022). «Корреляция между патогенными процессами фибромиалгии и синдромом раздраженного кишечника в популяции среднего возраста: систематический обзор» . Cureus . 14 (10): E29923. doi : 10.7759/cureus.29923 . PMC 9635936 . PMID 36381861 .
- ^ D'Onghia M, Ciaffi J, Lisi L, Mancarella L, Ricci S, Stefanelli N, et al. (Апрель 2021 г.). «Фибромиалгия и ожирение: комплексный систематический обзор и метаанализ». Семинары по артриту и ревматизму . 51 (2): 409–424. doi : 10.1016/j.semarthrit.2021.02.007 . PMID 33676126 . S2CID 232136088 .
- ^ Alsiri N, Alhadhoud M, Alkatefi T, Palmer S (февраль 2023 г.). «Сопутствующий диагноз фибромиалгии и нарушений соединительной ткани: систематический обзор» (PDF) . Семинары по артриту и ревматизму . 58 : 152127. DOI : 10.1016/j.semarthrit.2022.152127 . PMID 36462303 . S2CID 253650110 . Архивировано (PDF) из оригинала 7 января 2024 года . Получено 7 января 2024 года .
- ^ Kocyigit bf, Akyol A (март 2023 г.). «Сосуществование синдрома фибромиалгии и воспалительных ревматических заболеваний, а также автономное поражение сердечно -сосудистой системы при синдроме фибромиалгии». Клиническая ревматология . 42 (3): 645–652. doi : 10.1007/s10067-022-06385-8 . PMID 36151442 . S2CID 252496799 .
- ^ Он J (2024). «Фибромиалгия при обструктивном синдроме апноэ-гипопниа сна: систематический обзор и метаанализ» . Границы в физиологии . 15 doi : 10.3389/fphys.2024.1394865 . PMC 11144865 . PMID 38831795 .
- ^ Padhan P, Maikap D, Pathak M (2023). «Синдром беспокойной ноги в ревматических условиях: его распространенность и факторы риска, метаанализ» . Международный журнал ревматических заболеваний . 26 (6): 1111–1119. doi : 10.1111/1756-185x.14710 . ISSN 1756-1841 . PMID 37137528 . S2CID 258484602 . Архивировано из оригинала 28 июля 2023 года . Получено 28 июля 2023 года .
- ^ Голдберг Н., Тамам С., Вайнтрауб Ай (декабрь 2022 г.). «Связь между гиперактивным мочевым пузырями и фибромиалгией: систематический обзор и метаанализ». Международный журнал гинекологии и акушерства . 159 (3): 630–641. doi : 10.1002/ijgo.14290 . PMID 35641437 . S2CID 249236213 .
- ^ Sarzi-Puttini P, Atzeni F, Mease PJ (апрель 2011 г.). «Хроническая широко распространенная боль: от периферийной до центральной эволюции» . Лучшая практика и исследования. Клиническая ревматология . 25 (2): 133–139. doi : 10.1016/j.berh.2011.04.001 . ISSN 1532-1770 . PMID 22094190 .
- ^ Schmidt-Wilcke T, Clauw DJ (19 июля 2011 г.). «Фибромиалгия: от патофизиологии до терапии» . Природные обзоры. Ревматология . 7 (9): 518–527. doi : 10.1038/nrrheum.2011.98 . ISSN 1759-4804 . PMID 21769128 .
- ^ Jump up to: а беременный в дюймовый и D'Agnelli S, Redt-Nielsen L, Gerra MC, Zortorri K, Boggingai L, Baciarelo M, Bignami E (январь 2019 г.). «Fromyalgia: Genetics и Epigenenetics Insights может предоставить бас для разработки диагностических биомаркеров » Молекулярная боль 15 : 17448069819944. DOI : 10.1177/1744806988819944 . 6322092PMC PMID 30486733
- ^ Jump up to: а беременный в Ablin JN, Buskila D (февраль 2015 г.). «Обновление о генетике синдрома фибромиалгии». Лучшая практика и исследования. Клиническая ревматология . 29 (1): 20–28. doi : 10.1016/j.berh.2015.04.018 . PMID 26266996 .
- ^ Lee YH, Choi SJ, Ji JD, Song GG (февраль 2012 г.). «Кандидатские генные исследования фибромиалгии: систематический обзор и метаанализ». Ревматология International . 32 (2): 417–426. doi : 10.1007/s00296-010-1678-9 . PMID 21120487 . S2CID 6239018 .
- ^ Dutta D, Brummett CM, Moser SE, Fritche LG, Tsodikov A, Lee S, et al. (Май 2020). «Наследственность фенотипа фибромиалгии варьируется в зависимости от возраста» . Артрит и ревматология . 72 (5): 815–823. doi : 10.1002/art.41171 . PMC 8372844 . PMID 31736264 .
- ^ Jump up to: а беременный в Picnt AM, Luís M, Geenv Fra F, Lumley MA, Abris JN, Amris K, Buskil K, Busco D, Castelo-Branco M, Crofford LJ, Fitzcharles M, Полем нейробиологии и биобеторов Обзоры 151 : 105235 10.1016/j.neubiorev.2023.105235. HDL : 1874/4 ISSN 0149-7634 . PMID 37207842 . S2CID 258745974 .
- ^ Малетик В., Эрсон К.Л. (июнь 2009 г.). «Нейробиология депрессии, фибромиалгии и невропатической боли» . Границы в биологии . 14 (14): 5291–5338. doi : 10.2741/3598 . PMID 19482616 .
- ^ Jump up to: а беременный в Martins DF, Viseux FJ, Salm DC, Ribeiro AC, Da Silva HK, Seim LA, et al. (Декабрь 2021 г.). «Роль блуждающего нерва при синдроме фибромиалгии». Нейробиологии и биобиоэвиральные обзоры . 131 : 1136–1149. doi : 10.1016/j.neubiorev.2021.10.021 . PMID 34710514 . S2CID 239772451 .
- ^ Jump up to: а беременный Калейчева Н., Каллен А.Е., Эванс Р., Харрис Т., Николсон Т., Чалдер Т (январь 2021 г.). «Роль стрессоров жизни в фибромиалгии взрослых: систематический обзор и метаанализ исследований в области конкретного контроля» . Психологическая медицина . 51 (2): 177–193. doi : 10.1017/s0033291720004547 . PMID 33602373 . S2CID 231955641 .
- ^ Jump up to: а беременный в дюймовый и Юнг Й.Х., Ким Х, Ли Д., Ли Джи, Мун Дж.Ю., Чой Ш., Кан Д.Х. (январь 2021 г.). «Дисфункциональные энергетические метаболизмы при фибромиалгии по сравнению со здоровыми субъектами» . Молекулярная боль . 17 : 17448069211012833. DOI : 10.1177/17448069211012833 . PMC 8113919 . PMID 33940974 .
- ^ Schmidt-Wilcke T, Clauw DJ (июль 2011 г.). «Фибромиалгия: от патофизиологии до терапии». Природные обзоры. Ревматология . 7 (9): 518–527. doi : 10.1038/nrrheum.2011.98 . PMID 21769128 . S2CID 20678671 .
- ^ Casale R, Sarzi-Puttini P, Botto R, Alciati A, Batticciotto A, Marotto D, Torta R (январь 2019 г.). «Фибромиалгия и концепция устойчивости» . Клиническая и экспериментальная ревматология . 37 (1): 105–113. PMID 30747098 . Архивировано из оригинала 9 апреля 2022 года . Получено 9 апреля 2022 года .
- ^ Congratchano C, Marchi L, Rebecca C, Carmassi C, Contena B, Bazzichi LM, Gemignani A (28 сентября 2018 года). «Черты личности при фибромиалгии (FM): существует ли личность FM? Систематический обзор» . Клиническая практика и эпидемиология в области психического здоровья . 14 (1): 223–232. doi : 10.2174/1745017901814010223 . PMC 6166394 . PMID 30294356 .
- ^ Jump up to: а беременный Tan AC, Jaaniste T, чемпион D (5 мая 2019 г.). «Хроническая широко распространенная боль и синдром фибромиалгии: маркеры риска жизни в молодежи» . Исследование боли и управление . 2019 : 6584753. DOI : 10.1155/2019/6584753 . PMC 6525804 . PMID 31191788 .
- ^ Роуч К, Робертс Дж (август 2022 г.). «Комплексная сводка вариантов заболевания, вовлеченных в аллергию на металл» . Журнал токсикологии и здоровья окружающей среды Часть B: критические обзоры . 25 (6): 279–341. Bibcode : 2022jtehb..25..279r . doi : 10.1080/10937404.2022.2104981 . PMC 9968405 . PMID 35975293 . S2CID 251623384 .
- ^ Fialho MF, Brum ES, Oliveira SM (2023). «Может ли синдром фибромиалгии быть вызванным или усилением COVID-19?» Полем Воспалена . 31 (2): 633–651. doi : 10.1007/s10787-023-01160-w . ISSN 0925-4692 . PMC 9970139 . PMID 36849853 .
- ^ Де Томмазо М., Веккио Е., Нолано М (март 2022 г.). «Загадка фибромиалгии между синдромом центральной сенсибилизации и невропатией мелких волокон: повествовательный обзор о нейрофизиологических и морфологических данных». Неврологические науки . 43 (3): 1667–1684. doi : 10.1007/s10072-021-05806-x . PMID 35028777 . S2CID 245909381 .
- ^ Jump up to: а беременный Gkouvi A, Tsiogkas SG, Bogdanos DP, Gika H, Goulis DG, Grammatikopoulou Mg (23 апреля 2024 г.). «Протеомика у пациентов с синдромом фибромиалгии: систематический обзор наблюдательных исследований» . Текущая боль и головная боль отчетов . doi : 10.1007/s11916-024-01244-4 . ISSN 1531-3433 . PMC 11271354 . PMID 38652420 .
- ^ Den Boer C, Dries L, Terluin B, Van der Wouden JC, Blankenstein AH, Van Wilgen CP, et al. (Февраль 2019 г.). «Центральная сенсибилизация в хронической боли и необъяснимых исследования симптомов с медицинской точки зрения: систематический обзор определений, операционных и измерительных инструментов». Журнал психосоматических исследований . 117 : 32–40. doi : 10.1016/j.jpsychores.2018.12.010 . PMID 30665594 . S2CID 58565532 .
- ^ Bidari A, Ghavidel-Parsa B (октябрь 2022 г.). «Ноципластическая боль, механистическая основа для прагматического подхода к фибромиалгии». Клиническая ревматология . 41 (10): 2939–2947. doi : 10.1007/s10067-022-06229-5 . PMID 35701625 . S2CID 249650477 .
- ^ Nijs J, Lahousse A, Kapreli E, Bilika P, Saracoğlu İ, Malfliet A, et al. (Июль 2021 г.). «Критерии ноципластической боли или распознавание центральной сенсибилизации? Боли -фенотипирование в прошлом, настоящем и будущем» . Журнал клинической медицины . 10 (15): 3203. DOI : 10.3390/JCM10153203 . PMC 8347369 . PMID 34361986 .
- ^ Jump up to: а беременный Мартинес-Лавин М (декабрь 2018 г.). «Фибромиалгия и невропатия с небольшим волокном: участок сгущается!». Клиническая ревматология . 37 (12): 3167–3171. doi : 10.1007/s10067-018-4300-2 . PMID 30238382 . S2CID 52306843 .
- ^ Мартинес-Лавин М (февраль 2021 г.). "Ганглиазы дорсального корня: фабрика боли фибромиалгии?" Полем Клиническая ревматология . 40 (2): 783–787. doi : 10.1007/s10067-020-05528-z . PMC 7787228 . PMID 33409721 .
- ^ Jump up to: а беременный Мартинес-Лавин М., Холман А.Дж. (2021). «Анализ изменчивости сердечного ритма при ревматологии: прошлое, настоящее… и будущее?» Полем Клиническая и экспериментальная ревматология . 39 (5): 927–930. doi : 10.55563/clinexprheumatol/nmvth1 . PMID 34464245 . S2CID 237375381 .
- ^ Фигероа А., Кингсли Д.Д., Макмиллан В., Пантон Л.Б. (январь 2008 г.). «Тренировки для физических упражнений с сопротивлением улучшают изменчивость сердечного ритма у женщин с фибромиалгией» . Клиническая физиология и функциональная визуализация . 28 (1): 49–54. doi : 10.1111/j.1475-097x.2007.00776.x . PMID 18005081 . S2CID 40592827 .
- ^ Park HY, Jung WS, Kim J, Hwang H, Lim K (март 2020 г.). «Двенадцать недель аэробных упражнений на пороге лактата улучшают функцию вегетативной нервной системы, состав тела и аэробные показатели у женщин с ожирением» . Журнал ожирения и метаболического синдрома . 29 (1): 67–75. doi : 10.7570/jomes19063 . PMC 7118007 . PMID 32045515 .
- ^ Jump up to: а беременный Пинто А.М., Гинен Р., Вагер Т.Д., Ламли М.А., Хаузер В., Косек Е. и др. (Январь 2023 г.). «Регуляция эмоций и сеть значимости: гипотетическая интегративная модель фибромиалгии». Природные обзоры. Ревматология . 19 (1): 44–60. doi : 10.1038/s41584-022-00873-6 . HDL : 1874/426650 . PMID 36471023 . S2CID 254273384 .
- ^ Jump up to: а беременный в дюймовый Сингх Л., Каур А., Бхатти М.С., Бхатти Р. (июль 2019). «Возможные молекулярные медиаторы и механистическое понимание фибромиалгии и связанных сопутствующих заболеваний». Нейрохимические исследования . 44 (7): 1517–1532. doi : 10.1007/s11064-019-02805-5 . PMID 31004261 . S2CID 123945497 .
- ^ Jump up to: а беременный Беллато Е., Марини Е., Кастольди Ф., Барбасетти Н., Маттеи Л., Бонасия Д.Е., Блонна Д. (1 января 2012 г.). «Синдром фибромиалгии: этиология, патогенез, диагностика и лечение» . Исследование боли и лечение . 2012 : 426130. DOI : 10.1155/2012/426130 . PMC 3503476 . PMID 23213512 .
- ^ Jump up to: а беременный Feraco P, Bacci A, Pedrabissi F, Passamonti L, Zampogna G, Pedrabissi F, et al. (Октябрь 2011). «Метаболические аномалии в областях обезболивания пациентов с фибромиалгией: исследование 3T МР-спектроскопии» . Ajnr. Американский журнал нейрорадиологии . 32 (9): 1585–1590. doi : 10.3174/ajnr.a2550 . PMC 7965402 . PMID 21799042 .
- ^ Jump up to: а беременный Синь М., Ку -Й, Пенг Х, Чжу Д., Ченг С. (9 мая 2023 г.). «Систематический обзор и мета-анализ морфометрических исследований на основе вокселей» . Границы в нейробиологии . 17 doi : 10.3389/fnins.2023.1164145 . ISSN 1662-453x . PMC 10203234 . PMID 37229427 .
- ^ Jump up to: а беременный Лин С, Ли Ш. Ш., Вэн Х.Х. (1 января 2016 г.). «Атрофия серого вещества в сети по умолчанию фибромиалгии: метаанализ исследований морфометрии на основе вокселей» . Biomed Research International . 2016 : 7296125. DOI : 10.1155/2016/7296125 . PMC 5220433 . PMID 28105430 .
- ^ Jump up to: а беременный в дюймовый и Assavarittirong C, Samborski W, Grygiel-Górniak B (2022). «Окислительный стресс при фибромиалгии: от патологии к лечению» . Окислительная медицина и клеточная долговечность . 2022 : 1582432. DOI : 10.1155/2022/1582432 . PMC 9556195 . PMID 36246401 .
- ^ Coskun Benlidayi I (май 2019). «Роль воспаления в патогенезе и лечении фибромиалгии». Ревматология International . 39 (5): 781–791. doi : 10.1007/s00296-019-04251-6 . PMID 30756137 . S2CID 131775636 .
- ^ Jump up to: а беременный в Useyler N, Häuser W, Sommer C (октябрь 2011 г.). «Систематический обзор с мета-анализом: цитокины при синдроме фибромиалгии» . BMC скелетно -скелетные расстройства . 12 : 245. DOI : 10.1186/1471-2474-12-245 . PMC 3234198 . PMID 22034969 .
- ^ Jump up to: а беременный в Rodriguez-Pintó I, Agmon-Levin N, Howard A, Shoenfeld Y (октябрь 2014 г.). «Фибромиалгия и цитокины». Иммунологические письма . 161 (2): 200–203. doi : 10.1016/j.imlet.2014.01.009 . PMID 24462815 .
- ^ Dell'osso L, Bazzichi L, Baroni S, Falaschi V, Congrakano C, Carmassi C, Marazziti D (1 января 2015 г.). «Воспалительная гипотеза спектра настроения расширилась до синдрома фибромиалгии и хронической усталости». Клиническая и экспериментальная ревматология . 33 (1 Suppl 88): S109 - S116. PMID 25786052 .
- ^ Jump up to: а беременный Bazzichi L, Giacomelli C, Consensi A, Giorgi V, Batticciotto A, Franco M, Sarzi-Puttini P (2020). «Один год в обзоре 2020 года: фибромиалгия». Клиническая и экспериментальная ревматология . 38 (1): 3–8. PMID 32116216 .
- ^ Литтлджон G (ноябрь 2015). «Нейрогенное нейровоспаление при фибромиалгии и сложном региональном боли». Природные обзоры. Ревматология . 11 (11): 639–648. doi : 10.1038/nrrheum.2015.100 . PMID 26241184 . S2CID 4368913 .
- ^ Эрдрич С., Хаврак Д.А., Майерс С.П., Харнетт Дже (март 2020 г.). «Определение связи между фибромиалгией, кишечным микробиом и ее биомаркерами: систематический обзор» . BMC скелетно -скелетные расстройства . 21 (1): 181. DOI : 10.1186/S12891-020-03201-9 . PMC 7083062 . PMID 32192466 .
- ^ Wang Y, Wei J, Zhang W, Doherty M, Zhang Y, Xie H, et al. (Июнь 2022 г.). «Дисбиоз кишечника при ревматических заболеваниях: систематический обзор и метаанализ 92 обсервационных исследований» . ebiomedicine . 80 : 104055. DOI : 10.1016/j.ebiom.2022.104055 . PMC 9120231 . PMID 35594658 .
- ^ Minerbi A, Fitzcharles MA (январь 2020 г.). «Микробиом кишечника: уместность в фибромиалгии». Клиническая и экспериментальная ревматология . 38 (1): 99–104. PMID 32116215 .
- ^ Clos-Garcia M, Andrés-Marin N, Fernández-Eulate G, Abecia L, Lavín JL, Van Liempd S, et al. (Август 2019). «Анализ микробиомов кишечника и сыворотки идентифицирует молекулярные биомаркеры и измененный метаболизм глутамата при фибромиалгии» . ebiomedicine . 46 : 499–511. Doi : 10.1016/j.ebiom.2019.07.031 . PMC 6710987 . PMID 31327695 .
- ^ Borenstein D (апрель 1995 г.). «Распространенность и исход лечения первичной и вторичной фибромиалгии у пациентов с болью в позвоночнике». Позвоночник . 20 (7): 796–800. doi : 10.1097/00007632-199504000-00011 . PMID 7701393 . S2CID 30837539 .
- ^ Бенгтссон А., Анрикссон К.Г., Ларссон Дж (июль 1986 г.). «Снижение высокоэнергетических фосфатных уровней в болезненных мышцах пациентов с первичной фибромиалгией». Артрит и ревматизм . 29 (7): 817–821. doi : 10.1002/art.1780290701 . PMID 3741498 .
- ^ Gerdle B, Ghafouri B, Lund E, Bengtsson A, Lundberg P, Ettinger-Veenstra HV, et al. (Октябрь 2020 г.). «Свидетельство митохондриальной дисфункции при фибромиалгии: отклонение метаболизма мышечной энергии, обнаруженного с использованием микродиализа и магнитно -резонанса» . Журнал клинической медицины . 9 (11): 3527. DOI : 10.3390/JCM9113527 . PMC 7693920 . PMID 33142767 .
- ^ Srikuea R, Symons TB, Long DE, Lee JD, Shang Y, Chomentowski PJ, et al. (Февраль 2013 г.). «Ассоциация фибромиалгии с измененными характеристиками скелетных мышц, которые могут способствовать усталости после постдексерской усталости у женщин в постменопаузе» . Артрит и ревматизм . 65 (2): 519–528. doi : 10.1002/art.37763 . PMC 3558634 . PMID 23124535 .
- ^ Shang Y, Gurley K, Symons B, Long D, Srikuea R, Crofford LJ и др. (Ноябрь 2012). «Неинвазивная оптическая характеристика мышечного кровотока, оксигенации и метаболизма у женщин с фибромиалгией» . Исследование и терапию артрита . 14 (6): R236. doi : 10.1186/ar4079 . PMC 3674608 . PMID 23116302 .
- ^ Häuser W, Fitzcharles MA (март 2018 г.). «Факты и мифы, относящиеся к фибромиалгии» . Диалоги в клинической нейробиологии . 20 (1): 53–62. doi : 10.31887/dcns.2018.20.1/whauser . PMC 6016048 . PMID 29946212 .
- ^ Wolfe F (август 2003 г.). «Прекратите использовать Американский колледж критериев ревматологии в клинике» . Журнал ревматологии . 30 (8): 1671–1672. PMID 12913920 . Архивировано из оригинала 14 октября 2011 года.
- ^ Galvez-Sánchez CM, Reyes del Paso GA (апрель 2020 г.). «Диагностические критерии для фибромиалгии: критический обзор и перспективы будущих» . Журнал клинической медицины . 9 (4): 1219. DOI : 10.3390/JCM9041219 . PMC 7230253 . PMID 32340369 .
- ^ Ван С.М., Хан С., Ли С.Дж., Паткар А.А., Масанд П.С., Па -Ку (июнь 2015 г.). «Диагностика фибромиалгии: обзор прошлого, настоящего и будущего». Экспертный обзор нейротерапевтики . 15 (6): 667–679. doi : 10.1586/14737175.2015.1046841 . PMID 26035624 . S2CID 2412984 .
- ^ Burckhardt CS, Clark SR, Bennett RM (май 1991). «Анкета по фибромиалгии воздействия: развитие и проверка» . Журнал ревматологии . 18 (5): 728–733. PMID 1865419 . Архивировано из оригинала 16 мая 2022 года . Получено 18 июня 2022 года .
- ^ Jump up to: а беременный Беннетт Р.М., Друг Р., Джонс К.Д., Уорд Р., Хан Б.К., Росс Р.Л. (1 января 2009 г.). «Пересмотренная вопросник по воздействию фибромиалгии (FIQR): валидация и психометрические свойства» . Исследование и терапию артрита . 11 (4): R120. doi : 10.1186/ar2783 . PMC 2745803 . PMID 19664287 .
- ^ «Анкета по фибромиалгии воздействия (FIQ)» . Американский колледж ревматологии . Архивировано из оригинала 1 июля 2022 года . Получено 18 июня 2022 года .
- ^ Seidenberg M, Haltiner A, Taylor MA, Hermann BB, Wyler A (февраль 1994 г.). «Разработка и проверка вопросника с множественной способностью самоотчетов». Журнал клинической и экспериментальной нейропсихологии . 16 (1): 93–104. doi : 10.1080/01688639408402620 . PMID 8150893 .
- ^ Jump up to: а беременный в Goldenberg DL (декабрь 2009 г.). «Диагностика и дифференциальный диагноз фибромиалгии». Американский журнал медицины (обзор). 122 (12 Suppl): S14 - S21. doi : 10.1016/j.amjmed.2009.09.007 . PMID 19962492 .
- ^ Jump up to: а беременный в Häuser W, Perrot S, Sommer C, Shir Y, Fitzcharles MA (май 2017). «Диагностические факторы хронической широко распространенной боли: не всегда фибромиалгия» . Боль в отчетах . 2 (3): E598. doi : 10.1097/pr9.000000000000000598 . PMC 5741304 . PMID 29392213 .
- ^ Jump up to: а беременный Rossi A, Lollo AC, Guzzo MP, Giacomelli C, Atzeni F, Bazzichi L, Franco M (2015). «Фибромиалгия и питание: какие новости?». Клиническая и экспериментальная ревматология . 33 (1 Suppl 88): S117 -S125. PMID 25786053 .
- ^ Jump up to: а беременный Marchesoni A, De Marco G, Merashli M, McKenna F, Tinazzi I, Marzo-ortega H, McGonagle DG (январь 2018). «Проблема в дифференцировке между псориатическим политентезитом и фибромиалгией». Ревматология (обзор). 57 (1): 32–40. doi : 10.1093/ревматология/kex079 . PMID 28387854 . S2CID 205309871 .
- ^ Jump up to: а беременный Palazzi C, D'amico E, D'Engelo S, Gilio M, Olivieri I (январь 2016 г.). «Ревматические проявления хронической инфекции вируса гепатита С: показания для правильного диагноза» . Всемирный журнал гастроэнтерологии (обзор). 22 (4): 1405–1410. doi : 10.3748/wjg.v22.i4.1405 . PMC 4721975 . PMID 26819509 .
- ^ Jump up to: а беременный Sommer C, Häuser W, Alten R, Petzke F, Späth M, Tölle T, et al. (Июнь 2012 г.). «[Лекарственная терапия синдрома фибромиалгии. Систематический обзор, метаанализ и руководство]» (PDF) . Шмерц . 26 (3): 297–310. doi : 10.1007/s00482-012-1172-2 . PMID 22760463 . S2CID 1348989 . Архивировано из оригинала (PDF) 16 февраля 2013 года.
- ^ Jump up to: а беременный Фицчарлз М.А., Шир Й., Аблин Дж.Н., Бускила Д., Амитал Х, Хеннингсен П., Хаузер В. (2013). «Классификация и клиническая диагностика синдрома фибромиалгии: рекомендации недавних междисциплинарных руководств, основанных на фактических данных» . Основанная на фактических данных дополнительная и альтернативная медицина . 2013 : 528952. DOI : 10.1155/2013/528952 . PMC 3860136 . PMID 24379886 .
- ^ Jump up to: а беременный в «Управление | канадские руководящие принципы для диагностики и лечения фибромиалгии» . Архивировано из оригинала 11 июня 2013 года.
- ^ Busch AJ, Barber KA, Overend TJ, Peloso PM, Schachter CL (октябрь 2007 г.). «Упражнения для лечения синдрома фибромиалгии». Кокрановская база данных систематических обзоров (4): CD003786. doi : 10.1002/14651858.cd003786.pub2 . PMID 17943797 .
- ^ Jump up to: а беременный в Andrade A, Dominski FH, Sieczkowska SM (декабрь 2020 г.). «То, что мы уже знаем о влиянии физических упражнений у пациентов с фибромиалгией: обзор зонтика». Семинары по артриту и ревматизму . 50 (6): 1465–1480. doi : 10.1016/j.semarthrit.2020.02.003 . PMID 32147091 . S2CID 212638860 .
- ^ [ ненадежный медицинский источник? ] Masquelier E, D'Haeyere J (октябрь 2021 г.). «Физическая активность при лечении фибромиалгии». Суставный костный позвоночник . 88 (5): 105202. DOI : 10.1016/j.jbspin.2021.105202 . PMID 33962033 .
- ^ McLoughlin MJ, Stegner AJ, Cook DB (июнь 2011 г.). «Связь между физической активностью и реакциями мозга на боль при фибромиалгии» . Журнал боли . 12 (6): 640–651. doi : 10.1016/j.jpain.2010.12.004 . PMC 3111901 . PMID 21330218 .
- ^ Jump up to: а беременный Valim V, Natour J, Xiao Y, Pereira AF, Lopes BB, Pollak DF, et al. (Ноябрь 2013). «Влияние физических упражнений на уровни серотонина в сыворотке и его метаболита при фибромиалгии: рандомизированное пилотное исследование» . Revista Brasileira de Reumatologia (по -испански). 53 (6): 538–541. doi : 10.1016/j.rbr.2013.02.001 . PMID 24477734 .
- ^ Genc A, Tur BS, Aytur YK, Oztuna D, Erdogan MF (июль 2015 г.). «Влияют ли аэробные упражнения на гипоталамо-гипофизарный гормональный ответ у пациентов с синдромом фибромиалгии?» Полем Журнал науки о физиотерапии . 27 (7): 2225–2231. doi : 10.1589/jpts.27.2225 . PMC 4540854 . PMID 26311959 .
- ^ Jump up to: а беременный в дюймовый и фон El-Shewy KM, Kunbaz A, Down MM, Al-Hussein MJ, Saad AM, Sammour YM, Abdel-Daim PM (январь 2019). «Гипербарические кислородные и аэробные упражнения в долгосрочном лечении фибромилгии: повествовательный обзор » Биомедицина и фармакотерапия 109 : 629–6 Doi : 10.1016/ j.biopha.2018.10.1 30399600PMID S2CID 53240356
- ^ Андраде А., Виларино Г.Т., Сичковская С.М., Коимбра Д.Р., Стеффенс Р.А., Витта Г.Г. (март 2018 г.). «Острое влияние физических упражнений на маркеры воспаления пациентов с синдромом фибромиалгии: систематический обзор». Журнал нейроиммунологии . 316 : 40–49. doi : 10.1016/j.jneuroim.2017.12.007 . PMID 29254627 . S2CID 46879701 .
- ^ Jump up to: а беременный в дюймовый и фон глин Андраде А., Вилино Г.Т., Серафим Т.Т., Перейра Джуниор А.А., де Соуза С.А., Сичковская С.М. (Octber 2019). «Модуляция вегетативной функции с помощью физических упражнений у пациентов с синдромом фибромиалгии: систематический обзор». PM & R. 11 (10): 1121–1131. Doi : 10.1002/pmrj.12158 . PMID 30900831 . S2CID 85448644 .
- ^ Jump up to: а беременный в Albuquerque ML, Monteiro D, Marinho DA, Vilarino GT, Andrade A, Neiva HP (ноябрь 2022 г.). «Влияние различных протоколов физических упражнений на лечение синдрома фибромиалгии: систематический обзор и метаанализ рандомизированных контролируемых исследований». Ревматология International . 42 (11): 1893–1908. doi : 10.1007/s00296-022-05140-1 . HDL : 10400,8/7188 . PMID 35604435 . S2CID 248970279 .
- ^ Jump up to: а беременный в Estévez-López F, Maestre-Cascales C, Russell D, Alvarez-Gallardo IC, Rodriguez-Layllon M, Hughes CM, et al. (Апрель 2021 г.). «Эффективность физических упражнений в области усталости и качества сна при фибромиалгии: систематический обзор и метаанализ рандомизированных исследований» . Архив физической медицины и реабилитации . 102 (4): 752–761. doi : 10.1016/j.apmr.2020.06.019 . HDL : 10481/68683 . PMID 32721388 . S2CID 220847961 .
- ^ Cuenca-Martínez F, Suso-Martí L, Fernández-Carnero J, Muñoz-Alarcos V, Sempere-Rubio N (2023). «Вмешательства на основе физических упражнений на качество сна у пациентов с синдромом фибромиалгии: обзор зонтика и картирования с мета-анализом» . Семинары по артриту и ревматизму . 61 : 152216. DOI : 10.1016/j.semarthrit.2023.152216 . PMID 37229847 . S2CID 258597720 .
- ^ McVeigh JG, Lucas A, Hurley DA, Basford Jr, Baxter GD (сентябрь 2003 г.). «Восприятие пациентов в физиотерапии в лечении синдрома фибромиалгии: обследование». CORSLOSKELATE CARE . 1 (2): 98–107. doi : 10.1002/msc.45 . PMID 20217670 .
- ^ Jump up to: а беременный в Рассел Д., Альварес Галлардо И.К., Уилсон И., Хьюз С.М., Дэвисон Г.В., Санудо Б., Маквей Дж. Г. (март 2018 г.). « Упражнение для меня-страшное слово»: восприятие усталости, дисфункции сна и упражнения у людей с синдромом фибромиалгии-исследованием фокус-группы ». Ревматология International . 38 (3): 507–515. doi : 10.1007/s00296-018-3932-5 . PMID 29340774 . S2CID 3395036 .
- ^ Sanz-Boris Y, Pastor-Mircl. Полем Divertity и реабилитация 40 (21): 2475–2487. doi : 10.1080/ 0 PMID 286887050 . 9032840S2CID
- ^ Barhorst EE, Andrae WE, Rayne TJ, Falvo MJ, Cook DB, Lindheimer JB (декабрь 2020 г.). «Повышенное воспринимаемое усилие у людей с миалгическим энцефаломиелитом/синдромом хронической усталости и фибромиалгией: метаанализ» . Медицина и наука в спорте и упражнениях . 52 (12): 2615–2627. doi : 10.1249/mss.0000000000002421 . PMC 10200687 . PMID 32555018 . S2CID 219918068 .
- ^ Ванчампфорт Д., МакГрат Р.Л., Хеммингс Л., Гиллис В., Бернар К., Ван Дамм Т (ноябрь 2022 г.). «Физическая активность коррелирует у людей с фибромиалгией: систематический обзор» . Инвалидность и реабилитация . 45 (25): 4165–4174. doi : 10.1080/09638288.2022.2146911 . PMID 36398698 . S2CID 253627372 .
- ^ Райан С. (2013). «Уход за пациентами с фибромиалгией: оценка и лечение». Стандарт ухода . 28 (13): 37–43. doi : 10.7748/ns2013.11.28.13.37.e7722 . PMID 24279570 .
- ^ Majdoub F, Ben Nessib D, Ferjani HL, Kaffel D, Triki W, Maatallah K, Hamdi W (февраль 2023 г.). «Нефармакологическая терапия при фибромиалгии: новые горизонты для врачей, новые надежды на пациентов». CORSLOSKELATE CARE . 21 (3): 603–610. doi : 10.1002/msc.1741 . PMID 36757930 . S2CID 256696861 .
- ^ Bidonde J, Busch AJ, Schachter CL, Overend TJ, Kim Sy, Góes SM, et al. (Июнь 2017 г.). «Аэробные тренировочные тренировки для взрослых с фибромиалгией» . Кокрановская база данных систематических обзоров . 2017 (6): CD012700. doi : 10.1002/14651858.cd012700 . PMC 6481524 . PMID 28636204 .
- ^ Jump up to: а беременный Bidonde J, Busch AJ, Schachter CL, Webber SC, Musselman KE, Overend TJ, et al. (Май 2019). «Смешанная тренировка для взрослых с фибромиалгией» . Кокрановская база данных систематических обзоров . 2019 (5): CD013340. doi : 10.1002/14651858.cd013340 . PMC 6931522 . PMID 31124142 .
- ^ Ким Си, Буш А.Дж., Оверенд Т.Дж., Шахтер К.Л., Ван дер Спуи И., Боден С. и др. (Сентябрь 2019). «Тренировка гибкости для взрослых с фибромиалгией» . Кокрановская база данных систематических обзоров . 2019 (9): CD013419. doi : 10.1002/14651858.cd013419 . PMC 6718217 . PMID 31476271 .
- ^ Vilarino GT, Andreato LV, De Souza LC, Branco JH, Andrade A (ноябрь 2021 г.). «Влияние тренировок с сопротивлением на психическое здоровье пациентов с фибромиалгией: систематический обзор». Клиническая ревматология . 40 (11): 4417–4425. doi : 10.1007/s10067-021-05738-z . PMID 33987785 . S2CID 234489153 .
- ^ Родригес Аген-Саланг М., Чилли Р., Росалес-Тристанчо А 17 июля 2023 года). «Клиническая значимость обучения устойчивости у женщин с фибромиалгией: систематический обзор и метаанализ» . Журнал боли 28 (1): 21–3 doi : 10.1002/ejp.2161 . ISSN 1090-3 PMID 37458315 . 259949000S2CID
- ^ Bastos AC, Vilarino GT, De Souza LC, Dominski FH, Branco JH, Andrade A (15 мая 2023 г.). «Влияние тренировок с резистентностью на сон пациентов с фибромиалгией: систематический обзор» . Журнал психологии здоровья . 28 (11): 1072–1084. doi : 10.1177/13591053231172288 . ISSN 1359-1053 . PMID 37183814 . S2CID 258687258 . Архивировано из оригинала 28 июля 2023 года . Получено 28 июля 2023 года .
- ^ Jump up to: а беременный в дюймовый Da Silva JM, De Barros BS, Almeida GJ, O'Neil J, Imoto Am (март 2022 г.). «Дозировка упражнений с сопротивлением при фибромиалгии: синтез доказательств для систематического обзора литературы обновлен и метаанализ». Ревматология International . 42 (3): 413–429. doi : 10.1007/s00296-021-05025-9 . PMID 34652480 . S2CID 238991065 .
- ^ Li H, Chen J, Xu G, Duan Y, Huang D, Tang C, Liu J (сентябрь 2020 г.). «Влияние тай-чи на улучшение качества сна: систематический обзор и метаанализ». Журнал аффективных расстройств . 274 : 1102–1112. doi : 10.1016/j.jad.2020.05.076 . PMID 32663938 . S2CID 219743962 .
- ^ Vasileios P, Styliani P, Nifon G, Pavlos S, Aris F, Ioannis P (ноябрь 2022 г.). «Управление фибромиалгией с дополнительными и альтернативными медицинскими упражнениями: систематический обзор и метаанализ клинических испытаний». Ревматология International . 42 (11): 1909–1923. doi : 10.1007/s00296-022-05151-y . PMID 35796820 . S2CID 250317143 .
- ^ Cheng CA, Chiu YW, Wu D, Kuan YC, Chen Sn, Tam KW (октябрь 2019). «Эффективность тайцзи на пациентов с фибромиалгией: мета-анализ рандомизированных контролируемых исследований». Дополнительная терапия в медицине . 46 : 1–8. doi : 10.1016/j.ctim.2019.07.007 . PMID 31519264 . S2CID 199039433 .
- ^ Bidonde J, Busch AJ, Webber SC, Schachter CL, Danyliw A, Overend TJ, et al. (Октябрь 2014). «Водные тренировки для фибромиалгии» . Кокрановская база данных систематических обзоров . 2014 (10): CD011336. doi : 10.1002/14651858.cd011336 . PMC 10638613 . PMID 25350761 .
- ^ Lima TB, Dias JM, Mazuquin BF, Da Silva CT, Nogueira RM, Marques AP, et al. (Октябрь 2013). «Эффективность водной физиотерапии при лечении фибромиалгии: систематический обзор с мета-анализом». Клиническая реабилитация . 27 (10): 892–908. doi : 10.1177/0269215513484772 . PMID 23818412 . S2CID 25701866 .
- ^ Perraton L, Machotka Z, Kumar S (ноябрь 2009 г.). «Компоненты эффективных рандомизированных контролируемых исследований программ гидротерапии для синдрома фибромиалгии: систематический обзор» . Журнал исследований боли . 2 : 165–173. doi : 10.2147/jpr.s8052 . PMC 3004626 . PMID 21197303 .
- ^ Galvão-Moreira LV, De Castro LO, Moura EC, De Oliveira CM, Nogueira Neto J, Gomes LM, Leal Pd (июль 2021 г.). «Упражнения на основе бассейна для улучшения боли у взрослых с синдромом фибромиалгии: систематический обзор и метаанализ». Современная ревматология . 31 (4): 904–911. doi : 10.1080/14397595.2020.1829339 . PMID 32990113 . S2CID 222167851 .
- ^ Jump up to: а беременный Calles Plata I, Ortiz-Rubio A, Torres Sánchez I, Cabrera Martos I, Calvache Mateo A, Heredia-Ciuró A, Valenza MC (февраль 2023 г.). «Эффективность водной терапии во сне у людей с фибромиалгией. Метаанализ». Медицина сна . 102 : 76–83. doi : 10.1016/j.sleep.2022.12.016 . PMID 36603514 . S2CID 255217819 .
- ^ Ma J, Zhang T, Li X, Chen X, Zhao Q (сентябрь 2022 г.). «Влияние водной физиотерапии на клинические симптомы, физическую функцию и качество жизни у пациентов с фибромиалгией: систематический обзор и метаанализ». Теория и практика физиотерапии . 40 (2): 205–223. doi : 10.1080/09593985.2022.2119906 . PMID 36062580 . S2CID 252079586 .
- ^ Correyero-Leon M, Medrano-de-de-de-Fundent R, Hernando-Garijo I, Jiménez-Del-Barrrio S, Hernández-Lazaro H, Cebalos-Lazar-Laita L, Minga-Gomez Mt (Jul 2023). «Эффекты обучения поезда поезда водных поездов по аэробному и шагнущему экспериссу в счастье с фермером: системный обзор с мета-анализом » Исследуюсь 20 (1): 27–3 doi : 10.1016/j.explore . PMID 37460329 . 259580881S259580881
- ^ Bidonde J, Busch AJ, Van Der Spuy I, Tupper S, Kim Sy, Boden C (сентябрь 2017 г.). «Тренировки вибрации всего тела для фибромиалгии» . Кокрановская база данных систематических обзоров . 2017 (9): CD011755. doi : 10.1002/14651858.cd011755.pub2 . PMC 6483692 . PMID 28950401 .
- ^ «FDA одобряет первое препарат для лечения фибромиалгии» (пресс -релиз). США Управление по контролю за продуктами и лекарствами . 21 июня 2007 года. Архивировано из оригинала 21 февраля 2008 года . Получено 14 января 2008 года .
- ^ Европейское агентство лекарств. «Вопросы и ответы по рекомендации по отказу от авторизации маркетинга для Милнаципрана Пьера Фале Метекамента/Импультора» (PDF) . Европейское агентство лекарств. Архивировано (PDF) из оригинала 22 февраля 2014 года . Получено 30 мая 2013 года .
- ^ Martinez Je, Guimarãес I (февраль 2024 г.). « Фибромиалгия - Есть ли новые подходы?» . Best Pract Res Clin Rheumatol : 101933. DOI : 10.1016/j.berh.2024.101933 . PMID 38355316 .
- ^ Häuser W, Wolfe F, Tölle T, Useyler N, Sommer C (апрель 2012 г.). «Роль антидепрессантов в лечении синдрома фибромиалгии: систематический обзор и метаанализ». ЦНС лекарства . 26 (4): 297–307. doi : 10.2165/11598970-000000000-00000 . PMID 22452526 . S2CID 207301478 .
- ^ Cording M, Derry S, Phillips T, Moore RA, Wiffen PJ (октябрь 2015 г.). «Милнаципран от боли при фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 2015 (10): CD008244. doi : 10.1002/14651858.cd008244.pub3 . PMC 6481368 . PMID 26482422 .
- ^ Jump up to: а беременный Welsch P, üseyler N, Klose P, Walitt B, Häuser W (февраль 2018 г.). «Ингибиторы обратного захвата серотонина и норадреналина (SNRIS) для фибромиалгии» . Кокрановская база данных систематических обзоров . 2 (2): CD010292. doi : 10.1002/14651858.cd010292.pub2 . PMC 5846183 . PMID 29489029 .
- ^ Мур Р.А., Дерри С., Алдингтон Д., Коул П., Виффен П.Дж. (май 2019). «Амитриптилин для фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 5 (7): CD011824. doi : 10.1002/14651858.cd011824 . PMC 6485478 . PMID 35658166 .
- ^ Migliorini F, Maffulli N, Eschweiler J, Baroncini A, Bell A, Colarossi G (17 июля 2023 г.). «Дулоксетин для синдрома фибромиалгии: систематический обзор и метаанализ» . Журнал ортопедической хирургии и исследований . 18 (1): 504. doi : 10.1186/s13018-023-03995-z . ISSN 1749-799x . PMC 10351165 . PMID 37461044 .
- ^ Walitt B, Urrútia G, Nishishinya MB, Cantrell SE, Häuser W (июнь 2015 г.). «Селективные ингибиторы обратного захвата серотонина при синдроме фибромиалгии» . Кокрановская база данных систематических обзоров . 2015 (6): CD011735. doi : 10.1002/14651858.cd011735 . PMC 4755337 . PMID 26046493 .
- ^ Jump up to: а беременный Мур Р.А., Дерри С., Алдингтон Д., Коул П., Виффен П.Дж. (июль 2015 г.). «Амитриптилин для невропатической боли у взрослых» . Кокрановская база данных систематических обзоров . 2015 (7): CD008242. doi : 10.1002/14651858.cd011824 . PMC 6485478 . PMID 26146793 .
- ^ Welsch P, Bernardy K, Derry S, Moore RA, Häuser W (август 2018 г.). «Миразапин для фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 8 (8): CD012708. doi : 10.1002/14651858.cd012708.pub2 . PMC 6513659 . PMID 30080242 .
- ^ Jump up to: а беременный в Tort S, Urrútia G, Nishishinya MB, Walitt B (апрель 2012 г.). «Ингибиторы моноаминоксидазы (MAOI) для синдрома фибромиалгии». Кокрановская база данных систематических обзоров (4): CD009807. doi : 10.1002/14651858.cd009807 . PMID 22513976 .
- ^ Wiffen PJ, Derry S, Bell RF, Rice AS, Tölle TR, Phillips T, Moore RA (июнь 2017 г.). «Габапентин для хронической невропатической боли у взрослых» . Кокрановская база данных систематических обзоров . 6 (6): CD007938. doi : 10.1002/14651858.cd007938.pub4 . PMC 6452908 . PMID 28597471 .
- ^ Derry S, Cording M, Wiffen PJ, Law S, Phillips T, Moore RA (сентябрь 2016 г.). «Прегабалин от боли при фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 9 (9): CD011790. doi : 10.1002/14651858.cd011790.pub2 . PMC 6457745 . PMID 27684492 .
- ^ Straube S, Moore RA, Paine J, Derry S, Phillips CJ, Hallier E, McQuay HJ (июнь 2011 г.). «Вмешательство в работу в фибромиалгию: влияние лечения прегабалином и связь с обезболивающим ответом» . BMC скелетно -скелетные расстройства . 12 : 125. DOI : 10.1186/1471-2474-12-125 . PMC 3118156 . PMID 21639874 .
- ^ Nowell WB, Gavigan K, L Silverman S (май 2022). «Каннабис при боли ревматической болезни: обзор современной литературы». Текущие ревматологические отчеты . 24 (5): 119–131. doi : 10.1007/s11926-022-01065-7 . PMID 35486218 . S2CID 248423563 .
- ^ Boehnke KF, Häuser W, Fitzcharles MA (июль 2022 г.). «Каннабидиол (CBD) при ревматических заболеваниях (боль в опорно -двигательном скелете)» . Текущие ревматологические отчеты . 24 (7): 238–246. doi : 10.1007/s11926-022-01077-3 . PMC 9062628 . PMID 35503198 .
- ^ Бурк SL, Schlag AK, O'Sullivan SE, Nutt DJ, Finn DP (декабрь 2022 г.). «Каннабиноиды и эндоканнабиноидная система при фибромиалгии: обзор доклинических и клинических исследований» . Фармакология и терапия . 240 : 108216. DOI : 10.1016/j.pharmthera.2022.108216 . PMID 35609718 . S2CID 248973512 .
- ^ Jain N, Moorthy A (июнь 2022 г.). "Каннабиноиды в ревматологии: друг, враг или свидетель?" Полем CORSLOSKELATE CARE . 20 (2): 416–428. doi : 10.1002/msc.1636 . PMC 9322323 . PMID 35476898 .
- ^ Jump up to: а беременный Maclean AJ, Schwartz TL (май 2015). «Трамадол для лечения фибромиалгии». Экспертный обзор нейротерапевтики . 15 (5): 469–475. doi : 10.1586/14737175.2015.1034693 . PMID 25896486 . S2CID 26613022 .
- ^ Gaskell H, Moore RA, Derry S, Stannard C, et al. (Кокрановская боль, паллиативная и поддерживающая группа) (сентябрь 2016 г.). «Оксикодон от боли при фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 2016 (9): CD012329. doi : 10.1002/14651858.cd012329 . PMC 6457853 . PMID 27582266 .
- ^ Thorpe J, Shum B, Moore RA, Wiffen PJ, Gilron I (февраль 2018 г.). «Комбинированная фармакотерапия для лечения фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 2 (2): CD010585. doi : 10.1002/14651858.cd010585.pub2 . PMC 6491103 . PMID 29457627 .
- ^ Goldenberg DL, Clauw DJ, Palmer Re, Clair AG (май 2016 г.). «Использование опиоидов при фибромиалгии: предостерегающая история» . Майоневое разбирательство в клинике (обзор). 91 (5): 640–648. doi : 10.1016/j.mayocp.2016.02.002 . PMID 26975749 . S2CID 20228209 .
- ^ Бергер А. Модели использования опиоидов у пациентов с фибромиалгией в: Eular; 2009: SAT0461
- ^ Элайджа Дж., Пауэлл К., Смит М.А. (июнь 2022 г.). «Эффективность капсаицина в отношении качества сна и усталости при фибромиалгии». Журнал Pain & Palliateive Care Pharmacotherapy . 36 (2): 112–116. doi : 10.1080/15360288.2022.2063468 . PMID 35471125 . S2CID 248389141 .
- ^ Staud R (август 2011 г.). «Оксибат натрия для лечения фибромиалгии». Экспертное мнение о фармакотерапии . 12 (11): 1789–1798. doi : 10.1517/14656566.2011.589836 . PMID 21679091 . S2CID 33026097 .
- ^ См. S, Ginzburg R (август 2008 г.). «Выбор релаксанта скелетных мышц» . Американский семейный врач . 78 (3): 365–370. PMID 18711953 . Архивировано с оригинала 1 апреля 2016 года.
- ^ Кальтсас Г., Цивериотис К. (2000). «Фибромиалгия» . Endotext . MDText.com, Inc. PMID 25905317 . Архивировано из оригинала 6 августа 2020 года . Получено 20 февраля 2017 года .
- ^ Хейманн Р.Е., Пайва и, Хельфенштейн М., Поллак Д.Ф., Мартинес Дж., Прованс -младший и др. (2010). «Бразильский консенсус по поводу лечения фибромиалгии» . Revista Braziliira de Rheumatology . 50 (1): 56–66. Doi : 10.1590/s0482-5004201000000006 . PMID 21125141 .
- ^ Derry S, Wiffen PJ, Häuser W, Mücke M, Tölle TR, Bell RF, Moore RA (март 2017 г.). «Пероральные нестероидные противовоспалительные препараты для фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 3 (3): CD012332. doi : 10.1002/14651858.cd012332.pub2 . PMC 6464559 . PMID 28349517 .
- ^ Walitt B, Klose P, üceyler N, Phillips T, Häuser W (июнь 2016 г.). «Антипсихотики для фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 2016 (6): CD011804. doi : 10.1002/14651858.cd011804.pub2 . PMC 6457603 . PMID 27251337 .
- ^ Walitt B, Klose P, Fitzcharles MA, Phillips T, Häuser W (июль 2016 г.). «Каннабиноиды для фибромиалгии» . Кокрановская база данных систематических обзоров . 7 (7): CD011694. doi : 10.1002/14651858.cd011694.pub2 . PMC 6457965 . PMID 27428009 .
- ^ Jump up to: а беременный Kadayifci FZ, Bradley MJ, Onat AM, Shi Hn, Zheng S (ноябрь 2022 г.). «Обзор питательных подходов к фибромиалгии». Обзоры питания . 80 (12): 2260–2274. doi : 10.1093/utrit/nuac036 . PMID 35674686 .
- ^ Надаль-Николас и, Мираллес-Аморос Л., Мартинес-Ольцина М., Санчес-Ортега М., Мора Дж., Мартинес-Родригес А (май 2021). «Вегаран и Ванган диета при фибромиалгии: систематический обзор » . Международный журнал экологических исследований и общественного здравоохранения . 18 (9): 4955. DOI : 10.3390/ijerph18094955 . PMC 81255538 . PMID 34066603 .
- ^ Haddad HW, Mallepalli NR, Scheinuk JE, Bhargava P, Cornett EM, Urits I, Kaye AD (декабрь 2021 г.). «Роль питательных добавок в лечении хронической боли при фибромиалгии: повествовательный обзор» . Боль и терапия . 10 (2): 827–848. doi : 10.1007/s40122-021-00266-9 . PMC 8586285 . PMID 33909266 .
- ^ Jump up to: а беременный Qu K, Li MX, Zhou YL, Yu P, Dong M (апрель 2022 г.). «Эффективность витамина D в лечении фибромиалгии: метаанализ рандомизированных контролируемых исследований и систематический обзор». Экспертный обзор клинической фармакологии . 15 (4): 433–442. doi : 10.1080/17512433.2022.2081151 . PMID 35596576 . S2CID 248948241 .
- ^ Мехрабани С., Аскари Г., Мирахаджани М., Таваколи Р., Араб А (апрель 2019 г.). «Влияние добавок коэнзима Q10 на усталость: системный обзор интервенционных исследований» Дополнительная терапия в медицине 43 : 181–1 Doi : 10.1016/ j.ctim.2019.01.0 PMID 30935528 86467031S2CID
- ^ Hargreaves IP, Mantle D (2021). «Целевое лечение возрастной фибромиалгии с дополнительным коэнзимом Q10» (PDF) . В гостевом ПК (ред.). Отзывы о новых целях лекарств при возрастных расстройствах . Достижения в области экспериментальной медицины и биологии. Тол. 1286. Cham: Springer International Publishing. С. 77–85. doi : 10.1007/978-3-030-55035-6_5 . ISBN 978-3-030-55034-9 Полем PMID 33725346 . S2CID 232261388 . Архивировано (PDF) из оригинала 30 мая 2023 года . Получено 17 мая 2023 года .
- ^ Erkilic B, Dalgic GS (январь 2023 г.). «Профилактическая роль витамина D в профилактике и лечении синдрома фибромиалгии». Питание и здоровье . 29 (2): 223–229. doi : 10.1177/02601060221144801 . PMID 36591895 . S2CID 255471623 .
- ^ Jump up to: а беременный Hemati K, Amini Kadijani A, Sayehmiri F, Mehrzadi S, Zabihiyeganeh M, Hosseinzadeh A, Mirzaei A (февраль 2020 года). «Мелатонин в лечении симптомов фибромиалгии: систематический обзор». Дополнительная терапия в клинической практике . 38 : 101072. DOI : 10.1016/j.ctcp.2019.101072 . PMID 31783341 . S2CID 208497324 .
- ^ de Carvalho JF, Skare TL (2023). «Добавка мелатонина улучшает активность ревматологических заболеваний: систематический обзор» . Клиническое питание Espen . 55 : 414–419. doi : 10.1016/j.clnesp.2023.04.011 . PMID 37202076 . S2CID 258273314 . Архивировано из оригинала 5 января 2024 года . Получено 28 июля 2023 года .
- ^ Arnold LM, Gebke KB, Choy EH (февраль 2016 г.). «Фибромиалгия: стратегии управления для поставщиков первичной медицинской помощи» . Международный журнал клинической практики . 70 (2): 99–112. doi : 10.1111/ijcp.12757 . PMC 6093261 . PMID 26817567 .
- ^ Okifuji A, Hare BD (декабрь 2013 г.). «Управление синдромом фибромиалгии: обзор доказательств» . Боль и терапия . 2 (2): 87–104. doi : 10.1007/s40122-013-0016-9 . PMC 4107911 . PMID 25135147 .
- ^ Williams AC, Fisher E, Hearn L, Eccleston C (август 2020 г.). «Психологическая терапия для лечения хронической боли (исключая головную боль) у взрослых» . Кокрановская база данных систематических обзоров . 8 (8): CD007407. doi : 10.1002/14651858.cd007407.pub4 . PMC 7437545 . PMID 32794606 .
- ^ Бернарди К., Клоз П., Буш А.Дж., Чой Э.Х., Хаузер В. (сентябрь 2013 г.). «Когнитивно -поведенческая терапия при фибромиалгии» . Кокрановская база данных систематических обзоров . 2013 (9): CD009796. doi : 10.1002/14651858.cd009796.pub2 . PMC 6481397 . PMID 24018611 .
- ^ Jump up to: а беременный Glombiewski JA, Sawyer AT, Gutermann J, Koenig K, Rief W, Hofmann SG (ноябрь 2010 г.). «Психологическое лечение фибромиалгии: метаанализ». Боль . 151 (2): 280–295. doi : 10.1016/j.pain.2010.06.011 . PMID 20727679 . S2CID 10513179 .
- ^ Бернарди К., Фюбер Н., Кёллнер В., Хаузер В. (октябрь 2010). «Эффективность когнитивно -поведенческой терапии при синдроме фибромиалгии - систематический обзор и метаанализ рандомизированных контролируемых исследований» . Журнал ревматологии . 37 (10): 1991–2005. doi : 10.3899/jrheum.100104 . PMID 20682676 . S2CID 11357808 .
- ^ Jump up to: а беременный Whale K, Dennis J, Wylde V, Beswick A, Gooberman-Hill R (май 2022). «Эффективность нефармакологических вмешательств сна для людей с хронической болью: систематический обзор и метаанализ» . BMC скелетно -скелетные расстройства . 23 (1): 440. DOI : 10.1186/S12891-022-05318-5 . PMC 9092772 . PMID 35546397 .
- ^ Иствуд Ф., Годфри Е (12 декабря 2023 г.). «Эффективность, приемлемость и безопасность принятия и терапии приверженностью фибромиалгии-систематический обзор и метаанализ» . Британский журнал боли . 18 (3): 243–256. doi : 10.1177/20494637231221451 . ISSN 2049-4637 . PMC 11092929 . PMID 38751564 .
- ^ Suso-Martí L, Cuenca-Martínez F, Alba-Fenda P, Muñoz-Alarcos V, Herranz-Gómez A, Varangot-Reille C, et al. (Octaber 2022). «Эффективность обезболивающей нейронауки у пациентов с фибромиалгией: системный обзор и метаанализ». Обезболивающее лекарство . 23 (11): 1837–1850. Doi : 10.1093/pm/pnac077 . PMID 35587171 .
- ^ Duhn P, Wæhrens E, Pedersen M, Nielsen S, Locht H, Bliddal H, Christensen R, Amris K (10 мая 2023 г.). «Эффективность обучения пациентов как отдельное вмешательство для пациентов с хронической широко распространенной болью и фибромиалгией: систематический обзор и мета-анализ рандомизированных исследований» . Скандинавский журнал ревматологии . 52 (6): 654–663. doi : 10.1080/03009742.2023.2192450 . ISSN 0300-9742 . PMID 37162478 . S2CID 258588927 . Архивировано из оригинала 28 июля 2023 года . Получено 28 июля 2023 года .
- ^ Jump up to: а беременный Navarro-ledesma S, Hamed-Hamed D, Gonzalez-Muñoz A, Pruimboom L (2024). «Влияние методов физиотерапии и общих вмешательств на качество сна у пациентов с хронической болью: систематический обзор» . Обзоры медицины сна . 76 : 101937. DOI : 10.1016/j.smrv.2024.101937 . HDL : 10481/92720 . PMID 38669729 .
- ^ Theadom A, Cropley M, Smith HE, Feigin VL, McPherson K (апрель 2015 г.). «Терапия разума и тела при фибромиалгии» . Кокрановская база данных систематических обзоров . 2015 (4): CD001980. doi : 10.1002/14651858.cd001980.pub3 . PMC 8409283 . PMID 25856658 .
- ^ Deare JC, Zheng Z, Xue CC, Liu JP, Shang J, Scott SW, Littlejohn G (май 2013). «Акупунктура для лечения фибромиалгии» . Кокрановская база данных систематических обзоров . 2013 (5): CD007070. doi : 10.1002/14651858.cd007070.pub2 . PMC 4105202 . PMID 23728665 .
- ^ Cheng YC, Hsiao Cy, Su Mi, Chiu CC, Huang YC, Huang WL (февраль 2023 г.). «Лечение фибромиалгии электрической нейромодуляцией: систематический обзор и метаанализ». Клиническая нейрофизиология . 148 : 17–28. doi : 10.1016/j.clinph.2023.01.011 . PMID 36774784 . S2CID 256461558 .
- ^ Гикаро Дж. М., Багамбо Ф.М., Минде В.М., Сваи Э.А. (20 апреля 2023 г.). «Эффективность электрофизических агентов при фибромиалгии: систематический обзор и сетевой метаанализ» . Клиническая реабилитация . 37 (10): 1295–1310. doi : 10.1177/02692155231170450 . ISSN 0269-2155 . PMID 37082791 . S2CID 258258250 . Архивировано из оригинала 28 июля 2023 года . Получено 28 июля 2023 года .
- ^ Джонсон М.И., Клэйдон Л.С., Хербисон Г.П., Джонс Г., Пейли С.А. и др. (Кокрановская боль, паллиативная и поддерживающая группа) (октябрь 2017 г.). «Чернокожная электрическая стимуляция нерва (десятки) для фибромиалгии у взрослых» . Кокрановская база данных систематических обзоров . 2017 (10): CD012172. doi : 10.1002/14651858.cd012172.pub2 . PMC 6485914 . PMID 28990665 .
- ^ Jump up to: а беременный в Гибсон В., Уэнд Б.М., Мидс С., Кэтли М.Дж., О'Коннелл Н.Е. (апрель 2019). «Чернокожная стимуляция электрического нерва (десятки) для хронической боли - обзор кокрановских обзоров» . Кокрановская база данных систематических обзоров . 4 (4): CD011890. doi : 10.1002/14651858.cd011890.pub3 . PMC 6446021 . PMID 30941745 .
- ^ Jump up to: а беременный Lange G, Janal MN, Maniker A, Fitzgibbons J, Fobler M, Cook D, Natelson BH (сентябрь 2011 г.). «Безопасность и эффективность стимуляции блуждающего нерва при фибромиалгии: доказательство концепции фазы I/II» . Обезболивающее лекарство . 12 (9): 1406–1413. doi : 10.1111/j.1526-4637.2011.01203.x . PMC 3173600 . PMID 21812908 .
- ^ Gao C, Zhu Q, Gao Z, Zhao J, Jia M, Li T (октябрь 2022 г.). «Может ли неинвазивная стимуляция мозга улучшить боль и симптомы депрессии у пациентов с невропатической болью? Систематический обзор и метаанализ». Журнал боли и лечения симптомов . 64 (4): E203 - E215. doi : 10.1016/j.jpainsymman.2022.05.002 . PMID 35550165 . S2CID 248715312 .
- ^ Teixeira PE, Pacheco-Barrios K, Branco LC, De Melo PS, Marduy A, Caumo W, et al. (Ноябрь 2022 г.). «Анальгетический эффект транскраниальной стимуляции постоянного тока при фибромиалгии: систематический обзор, метаанализ и мета-регрессия потенциальных влиятельных лиц клинического эффекта» . Нейромодуляция . 26 (4): 715–727. doi : 10.1016/j.neurom.2022.10.044 . PMC 10203058 . PMID 36435660 . S2CID 253933442 .
- ^ Fernandes AM, Graven-Nielsen T, De Andrade DC (июнь 2022 г.). «Новые обновления транскраниальной магнитной стимуляции при хронической боли» . Текущее мнение о поддерживающей и паллиативной помощи . 16 (2): 65–70. doi : 10.1097/spc.000000000000000591 . PMID 35639571 . S2CID 249208885 .
- ^ Jump up to: а беременный в дюймовый Чу Ю.Дж., Квак С.Г., Чанг М.К. (июль 2022 г.). «Эффективность повторяющейся транскраниальной магнитной стимуляции при лечении фибромиалгии: систематический мета-анализ». Обезболивающее лекарство . 23 (7): 1272–1282. doi : 10.1093/pm/pnab354 . PMID 34983056 .
- ^ Jump up to: а беременный в дюймовый Sun P, Fang L, Zhang J, Liu Y, Wang G, Qi R (март 2022 г.). «Повторяющаяся транскраниальная магнитная стимуляция для пациентов с фибромиалгией: систематический обзор с мета-анализом». Обезболивающее лекарство . 23 (3): 499–514. doi : 10.1093/pm/pnab276 . PMID 34542624 .
- ^ Jump up to: а беременный Torres CB, Barona E, Manso J (2023). «Систематический обзор нейробиоуправления ЭЭГ при фибромиалгии для лечения психологических переменных, хронической боли и общего здоровья» . Европейские архивы психиатрии и клинической нейробиологии . 274 (4): 981–999. doi : 10.1007/s00406-023-01612-y . PMC 11127810 . PMID 37179502 .
- ^ Chen X, You J, Ma H, Zhou M, Huang C (январь 2023 г.). «Эффективность и безопасность гипербарической кислородной терапии для фибромиалгии: систематический обзор и метаанализ» . BMJ Open . 13 (1): E062322. doi : 10.1136/bmjopen-2022-062322 . PMC 9872467 . PMID 36690401 .
- ^ Jump up to: а беременный [ ненадежный медицинский источник? ] Б, Фицчарлз М.А., Хастт А.Л., Кац Р.С., Хаузер В., Вулф Ф. (октябрь 2011 г.). «Продольный результат фирреялгии: исследование 1555 пациентов » Журнал ревматологии 38 (10): 2238–2246. Doi : 10.3899/ jrheum.110026 21765102PMID S2CID 207672626
- ^ [ ненадежный медицинский источник? ] Kashikar-Zuck S, Cunningham N, Peugh J, Black WR, Nelson S, Lynch-Jordan AM и др. (Февраль 2019 г.). «Долгосрочные результаты подростков с фибромиалгией в возрасте от юношеских, в возрасте от юношеской, в взрослом возрасте и влияние депрессивных симптомов на функционирование с течением времени» . Боль . 160 (2): 433–441. doi : 10.1097/j.pain.0000000000001415 . PMC 6344278 . PMID 30335681 .
- ^ Leino-Arjas P, Rajaleid K, Mekuria G, Nummi T, Virtanen P, Hammarström A (январь 2018 г.). «Траектории опорно-двигательной боли от подросткового до среднего возраста: роль симптомов раннего депрессии, 27-летняя наблюдение северной шведской когорты». Боль . 159 (1): 67–74. doi : 10.1097/j.pain.0000000000001065 . PMID 28937577 . S2CID 22164186 .
- ^ Meuser T, Pietruck C, Radbruch L, Stute P, Lehmann Ka, Grond S (сентябрь 2001 г.). «Симптомы во время лечения боли в раке после Guidelines: продольное последующее исследование распространенности симптомов, тяжести и этиологии». Боль . 93 (3): 247–257. doi : 10.1016/s0304-3959 (01) 00324-4 . PMID 11514084 . S2CID 25457728 .
- ^ Treister-Goltzman Y, Peleg R (2023). «Фибромиалгия и смертность: систематический обзор и метаанализ» . RMD открытый . 9 (3): E003005. doi : 10.1136/rmdopen-2023-003005 . PMC 10335452 . PMID 37429737 . S2CID 259502501 .
- ^ Heidari F, Afshari M, Moosazadeh M (сентябрь 2017 г.). «Распространенность фибромиалгии у населения в целом и пациентов, систематический обзор и метаанализ» . Ревматология International . 37 (9): 1527–1539. doi : 10.1007/s00296-017-3725-2 . ISSN 0172-8172 . PMID 28447207 . S2CID 5043754 .
- ^ Wolfe F, Walitt B, Perrot S, Rasker JJ, Häuser W (13 сентября 2018 года). Соммер С (ред.). «Диагностика фибромиалгии и смещенная оценка: пол, распространенность и смещение» . Plos один . 13 (9): E0203755. BIBCODE : 2018PLOSO..1303755W . doi : 10.1371/journal.pone.0203755 . ISSN 1932-6203 . PMC 6136749 . PMID 30212526 .
- ^ Jump up to: а беременный D'Onghia M, Ciaffi J, Ruscitti P, Cipriani P, Giacomelli R, Ablin JN, Ursini F (октябрь 2022). «Экономическое бремя фибромиалгии: систематический обзор литературы». Семинары по артриту и ревматизму . 56 : 152060. DOI : 10.1016/j.semarthrit.2022.152060 . PMID 35849890 . S2CID 250271053 .
- ^ Беренсон А (14 января 2008 г.). "Препарат одобрено. Болезнь реальна?" Полем New York Times . Архивировано из оригинала 10 мая 2015 года . Получено 26 марта 2014 года .
- ^ «Фибромиалгия: интервью с доктором Фредериком Вулфом, Медицинской школой Канзасского университета» . 22 марта 2013 года. Архивировано с оригинала 29 мая 2014 года . Получено 28 мая 2014 года .
- ^ Goldenberg DL (январь 1995 г.). "Фибромиалгия: почему такой спор?" Полем Анналы ревматических заболеваний . 54 (1): 3–5. doi : 10.1136/ard.54.1.3 . PMC 1005499 . PMID 7880118 .
- ^ Hadlandsmyth K, Dailey DL, Rakel BA, Zimmerman MB, Vance CG, Merriwether EN, et al. (Май 2020). «Представления соматических симптомов у женщин с фибромиалгией по -разному связаны с повышенной депрессией и тревогой» . Журнал психологии здоровья . 25 (6): 819–829. doi : 10.1177/1359105317736577 . PMC 6287969 . PMID 29076404 .
- ^ Юнус М.Б. (июнь 2007 г.). «Фибромиалгия и перекрывающиеся расстройства: объединяющая концепция синдромов центральной чувствительности». Семинары по артриту и ревматизму . 36 (6): 339–356. doi : 10.1016/j.semarthrit.2006.12.009 . PMID 17350675 .
Внешние ссылки
[ редактировать ]- Артрит - типы - фибромиалгия по CDC
- Фибромиалгия Национального института артрита и опорно -двигательного аппарата и кожных заболеваний
- Фибромиалгия Американского колледжа ревматологии
- Фибромиалгия NHS